

I MUST SAY THAT THIS DESCRIBES MOST OF MY PAIN. I HAD TO RE-POST THIS, FOR I RAN ACROSS IT AGAIN ON THE NET AND IT SPOKE TO ME OF MY PAIN. IT DESCRIBED IT TO A T. I JUST WANT THIS NIGHTMARE TO END AND I KNOW THAT THERE IS HELP FOR ME SOMEWHERE, BUT I CAN'T FIND IT.:(((
IT SEEMS TO BE TRUE WHAT DR.OZ SAID ON TV THE OTHER DAY, WHEN HE SAID THAT DOCTORS JUST DON'T KNOW PAIN. THEY KNOW OF AREAS OF THE BODY, BUT THEY CAN'T PINPOINT WHERE PAIN IS COMING FROM USUALLY. THEY ARE NOT SPECIALIZING IN PAIN. THERE IS A SHORTAGE OF DOCTORS WHO DO. I TOTALLY AGREE WITH HIM AND IT IS A SAD WORLD WHERE SO MANY PEOPLE ARE SUFFERING. JUST LOOK IT UP AND TYPE IN THE WORD PAIN...AND U WILL SEE IT TOO. IT IS EVERYWHERE LIKE SOME EPIDEMIC OF PORPORTION.
EVERYONE NEEDS TO TRY TO UNDERSTAND THAT WE ALL HAVE OUR PROBLEMS, SOME SMALL AND SOME OVERWHELMING, BUT WE HAVE TO KEEP ON FIGHTING AND KEEP ON TRYING TO LIVE AND MOST DEFINITELY FEEL BLESSED IF U CAN ENJOY LIFE AND GIVE LOVE TO OTHERS, TO MAKE EVERYONE HAPPY OR TRY AT LEAST TO. SOME OF US, CAN'T CONTROL HOW WE FEEL...IT IS JUST THE WAY IT IS. IT WOULD BE A WONDERFUL THING, IF I COULD BE PAIN FREE. I WOULD LOVE THAT. THE FIRST THING, I WOULD DO IS ROUND UP MY BOYS AND GO FISHING. I HAVE WANTED TO DO THAT FOR SO LONG, BUT IT WASN'T IN THE CARDS FOR ME. I AM HONESTLY A BROKEN PERSON, NOT MY SPIRIT THOUGH...JUST MY BODY AND IT SEEMS THAT MY BODY ISN'T GETTING FIXED OR REPAIRED. NO, IT ONLY IS SEEMING TO GET WORSE AS TIME GOES ON, BUT I AM FIGHTING AND AM A FIGHTER. ONE DAY MY FIGHT WILL BE OVER, I PRAY. I AM TRYING TO MAKE IT, BUT IT IS EVER SO HARD.
I KNOW ,THAT WHAT I HAVE, IS BAD..BECAUSE NO ONE IS GETTING ME WELL AND I AM TIRED OF TRAVELING TO DOCS AND IT JUST SEEMS TO BE GETTING HARDER AND HARDER, FOR ME.
I KNOW ,THAT WHAT I HAVE, IS BAD..BECAUSE NO ONE IS GETTING ME WELL AND I AM TIRED OF TRAVELING TO DOCS AND IT JUST SEEMS TO BE GETTING HARDER AND HARDER, FOR ME.
I WANTED TO HAVE A WAY OF DOCUMENTING ALL THAT I GO THROUGH...BECAUSE I HAVE SO MANY SYMPTOMS...THAT AT TIME, I HAVE EVEN BEEN TOTALLY NUMB...ON THE WHOLE LEFT SIDE ONLY, I CAN SAY THAT AT THE TIME, I THOUGHT I WAS HAVING A STROKE OR HEART ATTACK, BECAUSE MY HEART-RATE WAS FAST, PINS/NEEDLES, NUMBNESS....AND MY FACE FELT LIKE IT WAS PULLING DOWN.
...BUT I DIDN'T EXPECT TO DO THIS...WRITE A BLOG. I DIDN'T WANT TO SEEM LIKE I WAS BEING DRAMATIC...I AM NOT. I AM JUST STATING THE FACTS, AS IT IS...I AM BEING REAL.
AS I SAID EARLIER, LIFE IS HARD, BUT WE HAVE TO KEEP ON FIGHTING AND I AM...LORD KNOWS, BUT I AM NOT PERFECT, BY NO MEANS. I AM ONLY HUMAN, BOUND TO MAKE MISTAKES...AS US ALL. I WILL SAY THAT TO ALL OF U THAT IF, U CAN CHANGE UR LIFE FOR THE BETTER AND IT IS OBTAINABLE...DO IT, BUT SOMETIMES, WE CAN'T CONTROL WHAT HAPPENS TO US OR WHY THINGS ARE THE WAY THEY ARE. IT WOULD BE NICE TO BE ABLE TO CONTROL WHAT AILS U...OR EVEN TROUBLES U.:)))<3
...BUT I DIDN'T EXPECT TO DO THIS...WRITE A BLOG. I DIDN'T WANT TO SEEM LIKE I WAS BEING DRAMATIC...I AM NOT. I AM JUST STATING THE FACTS, AS IT IS...I AM BEING REAL.
AS I SAID EARLIER, LIFE IS HARD, BUT WE HAVE TO KEEP ON FIGHTING AND I AM...LORD KNOWS, BUT I AM NOT PERFECT, BY NO MEANS. I AM ONLY HUMAN, BOUND TO MAKE MISTAKES...AS US ALL. I WILL SAY THAT TO ALL OF U THAT IF, U CAN CHANGE UR LIFE FOR THE BETTER AND IT IS OBTAINABLE...DO IT, BUT SOMETIMES, WE CAN'T CONTROL WHAT HAPPENS TO US OR WHY THINGS ARE THE WAY THEY ARE. IT WOULD BE NICE TO BE ABLE TO CONTROL WHAT AILS U...OR EVEN TROUBLES U.:)))<3
I FEE THAT A PERSON SHOULD FEEL BLESSED, IN ANY SITUATION...FOR, THE LORD IS WATCHING OVER US ALL AND IT IS OUR CHOICE TO LIVE FOR HIM...AS WE SHOULD.
HE DIED FOR US AND WE SHOULD BE GRATEFUL OF HIS SACRIFICE THAT WAS GIVEN...FOR ALL OF US.
HE DIED FOR US AND WE SHOULD BE GRATEFUL OF HIS SACRIFICE THAT WAS GIVEN...FOR ALL OF US.
SO, LIFE IS HARD...IF, WE LET IT BE. SOME OF US...ARE LIVING A HARD LIFE BECAUSE OF FACTORS...OUT OF OUR CONTROL....LIKE, OUR HEALTH.
IN THE END, IF WE KEEP THE LORD ALWAYS AT OUR SIDE...WE WILL BE ETERNALLY GRATEFUL.:)))
IN THE END, IF WE KEEP THE LORD ALWAYS AT OUR SIDE...WE WILL BE ETERNALLY GRATEFUL.:)))
GOD BLESS ALL OF U AND THANK U FOR ANY PRAYERS 4 ME.:D <3 Karen

THIS BELOW IS A RE-POST, BUT IT IS SO COMPELLING THAT I HAD TO. JUST READ IT AND U WILL SEE WHERE PAIN COMES FROM: (I have 18 of them and that is almost ALL of them)
(Sorry printing is so small on these first few listings, but lettering gets larger and easier to read. I don't know why it is doing that, when looks perfectly fine before post.)
Neck and Head Pain is the most common expression of myofascial dysfunction yet chronic headache sufferers respond badly to diagnoses of muscle tension headache. The labels of "vascular" headache or "neurological disease" seem more respectable, more likely to be taken seriously. But "vascular" doesn't stop at the head; "neurological" isn't restricted to the brain or spine. Tight muscles and fascia press, shear, block, and strangle both blood vessels and nerves throughout the body. “Muscle tension headache” can mean very simply “headache due to tight muscles” but from there it has been a short trip to “You’re just tense” and . . . “Have you considered psychiatric counseling?” with the clear implication that...
The pain is not real. YOU are just crazy.
Many pains do indeed have psychiatric components, but the psychogenic diagnosis is woefully overdone. Strangely, it is rarely applied to knee pain, big toe pain, or shoulder pain, but is used all too often by the physician, who, when asked for the underlying cause of head pain, cannot bring himself to say “I don’t know.” And there's a lot to know. Over 20 muscles (primarily of the neck) refer pain to the head. Several refer pain specifically to the eye. At least three refer pain directly to the teeth for reasons that will never be relieved by fillings or repeated root canals.
Of particular concern is strain or compression of the trigeminal nerve and its branches which mediate tissue inflammation, vasodilation and vascular permeability -- all issues in migraine. Over the last few years, plastic surgeons have verified the muscle-migraine connection beginning with the odd observation that Botox injections in the frontalis and corrugator muscles of the brow also eliminated migraines.
If irritated muscles and nerves fire off an inflammatory response and vasodilation, is the resulting headache "muscular," "neurological," or "vascular"? Perhaps the only real answer is "all of the above" because amazingly enough, it all functions together -- or dysfunctions together.
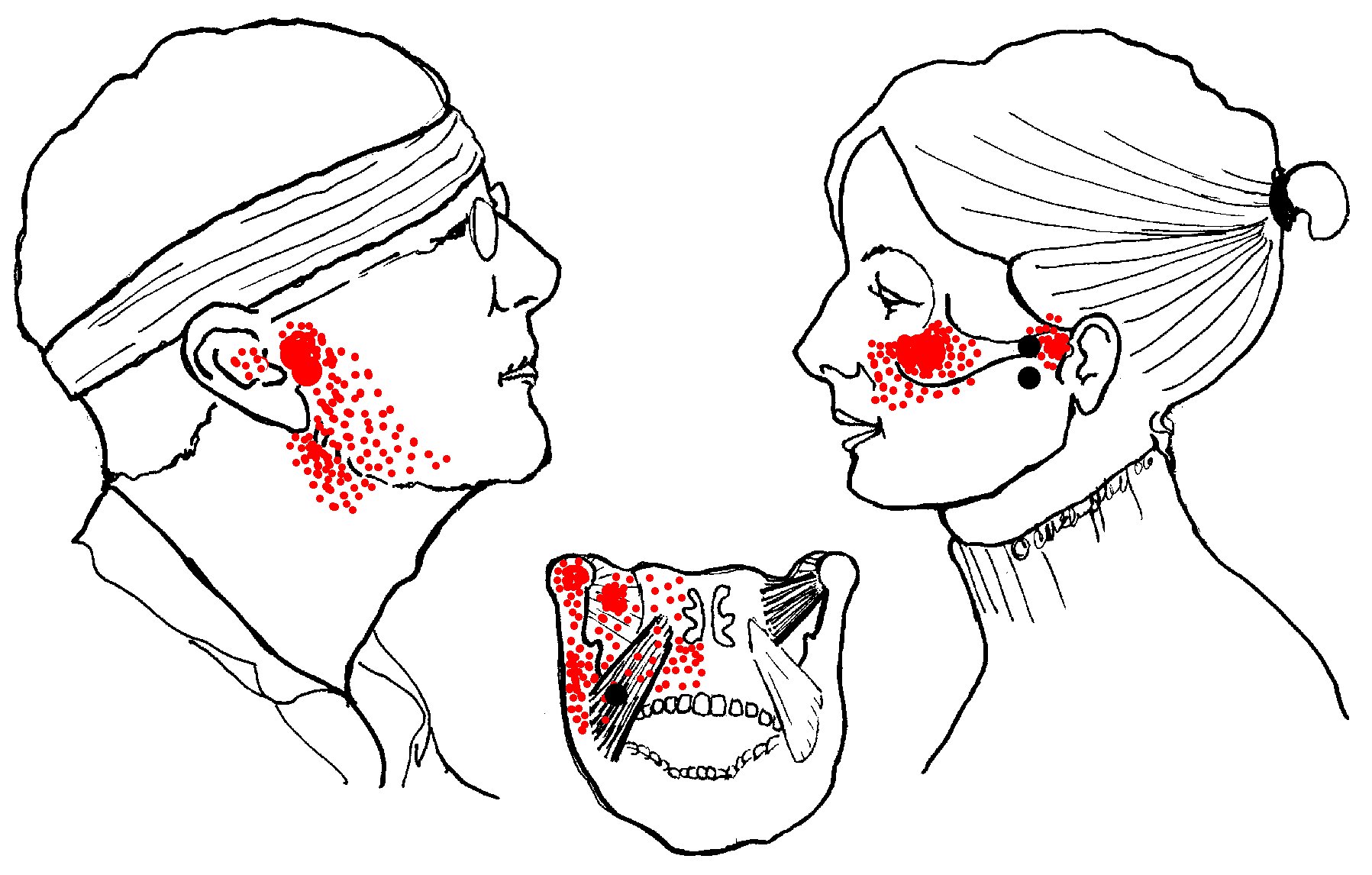
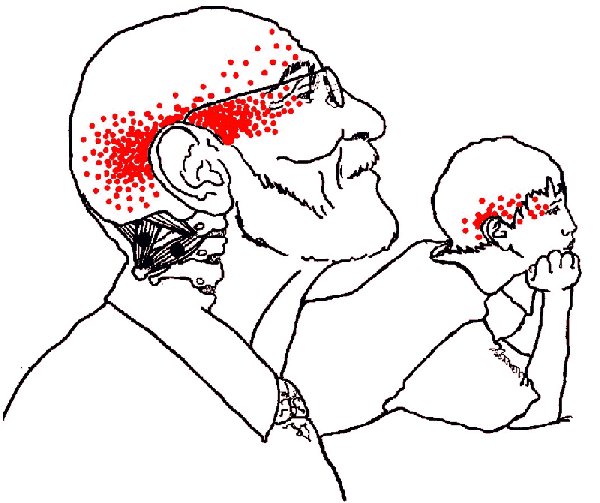
For patient or physician, the following pain patterns may look surprisingly familiar and will, we hope, point the user in the direction of truly effective treatment. In the following illustrations, black dots indicate common trigger point locations; red areas indicate the pain referred by the trigger point. You can evaluate these muscles with the Cervical and Masticatory Tests excerpted and adapted from our Range-of-Motion Testing Charts.
- Upper Trapezius > Tension headache and "bursitis". The trapezius muscle of the back and neck is the single muscle most likely to have trigger points in both adults and children.
 The upper trapezius refers a "fish-hook" pain pattern up the back side of the neck to the head, and around the temple to the eye. There may be goosebumps to upper arm and thigh possibly with nausea and visual disturbances. Problems often begin with heavy bags or purses, balancing phones between head and shoulder, or imbalances and strain by tight SCM or scalene muscles.
The upper trapezius refers a "fish-hook" pain pattern up the back side of the neck to the head, and around the temple to the eye. There may be goosebumps to upper arm and thigh possibly with nausea and visual disturbances. Problems often begin with heavy bags or purses, balancing phones between head and shoulder, or imbalances and strain by tight SCM or scalene muscles.
The nauseating pain of a one-sided trapezius headache is commonly diagnosed as "migraine" although migraine medications often fail to relieve the pain. ("Bursitis" and backpain may arise from the upper and lower fibers of the same muscle; see Introduction to Shoulder Pain.) - Sternocleidomastoid (SCM) >
 Dizziness, nausea, "migraine" and "sinus". Because of its intimate involvement with brain stem and the vagus nerve, the SCM muscle of the neck produces a long list of neurological and pain symptoms which appear primarily in the head and face but which may also appear as nausea, motion sickness, and balance problems. These are commonly mistaken for migraine, sinus headache, inner-ear problems, trigeminal neuralgia -- and so on. SCM has one of the most extensive patterns of pain and dysfunction, yet is one of the easiest muscles to self-treat. Click the link to see an info page on this muscle.
Dizziness, nausea, "migraine" and "sinus". Because of its intimate involvement with brain stem and the vagus nerve, the SCM muscle of the neck produces a long list of neurological and pain symptoms which appear primarily in the head and face but which may also appear as nausea, motion sickness, and balance problems. These are commonly mistaken for migraine, sinus headache, inner-ear problems, trigeminal neuralgia -- and so on. SCM has one of the most extensive patterns of pain and dysfunction, yet is one of the easiest muscles to self-treat. Click the link to see an info page on this muscle. - Scalenes > "Thoracic outlet" and "carpal tunnel" syndromes; chest, arm, and upper back pain. Scalenes contribute to severe tension headache and are one of the leading causes of "carpal tunnel syndrome." On the list of a half-dozen possible causes, the carpal tunnel itself is dead last. This is one of the reasons why carpal tunnel surgery is so ineffective. Check before you cut!
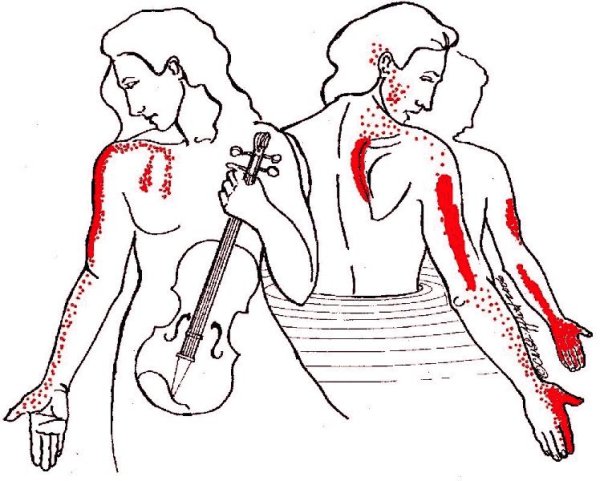
Notice also the fingerlike projections of pain extending down the chest. This is easily confused with angina. If you think you are having heart problems, get to a doctor immediately!
If, however, no cardiac problems are found, consider other muscles, especially if the chest pain was accompanied by a tingly thumb or index finger. Scalene pain typically extends down the upper arm, skipping the elbow. There may also be severe pain at the vertebral border of the scapula.
All of these patterns may be painfully familiar to wrestlers and Aikidoists who have suffered too many "neck-a-nage's." In Aikido, students who don't understand kokyu-nage techniques (based on balance and timing) tend to interpret what they think they see as: "Swing your partner around by the neck then drop him on his head," a painful variation on the game of “Hangman.”
In professional football, doing the same thing to a large, padded, extremely fit refrigerator-sized opponent by grabbing his face-guard will get you an instant 15-yard penalty, for very good reason.
The consequences of “neck-a-nage” can be extremely painful or disabling. The the electrical supply for arm and fingers comes from the brachial plexus, the “wiring harness” originating in the neck. If the source of finger pain is diagnosed as entrapment of the median nerve, the patient may be referred for carpal tunnel surgery. If the problem is identified as scalene entrapment of the brachial plexus, the current treatment is surgical removal("scalenectomy") of the anterior scalene and the first rib to which the muscle is attached. Unfortunately, this barbaric surgery usually causes more problems than it cures. Where care, consideration, and technical skill on the mat have failed, know this pain pattern and how to treat it -- by treating the muscle and its trigger points. - Masseter > TMJ, tinnitus, "sinus", and toothache. For its size and weight, the masseter is the strongest muscle in the body and its effects are not trivial.
 It refers pain to both upper and lower molar teeth, causes TMJ dysfunction, earache and a "sinus" pain over the eyebrow. Prozac and related anti-depressants such as Paxil specifically cause tightness in this muscle. If you're grinding your teeth at night and waking with a headache, ask your doctor about taking the medication during the daytime when you can be more aware of clenching and tooth-grinding which tense the masseter but also strain the temporalis . . .
It refers pain to both upper and lower molar teeth, causes TMJ dysfunction, earache and a "sinus" pain over the eyebrow. Prozac and related anti-depressants such as Paxil specifically cause tightness in this muscle. If you're grinding your teeth at night and waking with a headache, ask your doctor about taking the medication during the daytime when you can be more aware of clenching and tooth-grinding which tense the masseter but also strain the temporalis . . . - Temporalis > "Tension / sinus" headache, TMJ and toothache in upper teeth.
 Combine a head-forward position with a pipe and long hours of playing the violin (see the scalene pain pattern, above) and what do you get? "Elementary!" cries Dr. Watson. "Head pain, tooth pain, and extreme tooth sensitivity to heat/cold and vibration."
Combine a head-forward position with a pipe and long hours of playing the violin (see the scalene pain pattern, above) and what do you get? "Elementary!" cries Dr. Watson. "Head pain, tooth pain, and extreme tooth sensitivity to heat/cold and vibration."
You may wisely eschew "The Seven Percent Solution" in favor of directions to massage the temples to relieve tension headaches. But to make it more effective, notice the location of the trigger points and their specific areas of pain. Temporalis is remarkable for spoke-like lines of pain up into the temple and down into the upper teeth. Follow these lines and you will feel distinct taut bands. Massaging them may provide temporary relief. But the best approach is to follow the taut bands down to their trigger points located as shown near the cheekbones and adjacent to the ears.
- s > TMJ and "sinus" pain. The lateral pterygoids (at right) help to open and protrude the jaw. These relatively weak muscles are easily strained in opposing the powerful masseter and temporalis muscles that close the jaw.
The pterygoids commonly develop trigger points which in turn cause pain and/or clicking in the TMJ joint. They may block drainage from the maxillary sinus causing more still more pain. They are also linked to tinnitis, and cause lateral deviation on opening the jaw. There may be entrapment of the buccal nerve causing numbness / tingling in the cheek (see buccinator, below). The masseter muscle and medial pterygoid support the jaw like a sling. Masseter is on the outside, medial pterygoid inside; together they close the jaw.
 Medial pterygoids produce diffuse pain in the mouth involving the floor of the nose, tongue, throat and hard palate; pain below and behind the TMJ joint, pain and/or stuffiness of the ear, difficulty swallowing, lateral deviation and possibly pain on opening the jaw. They can also entrap the lingual nerve producing the odd symptom of a bitter, metallic taste in the mouth (which the patient may not connect with other symptoms and may not report for fear of being thought "crazy.")
Medial pterygoids produce diffuse pain in the mouth involving the floor of the nose, tongue, throat and hard palate; pain below and behind the TMJ joint, pain and/or stuffiness of the ear, difficulty swallowing, lateral deviation and possibly pain on opening the jaw. They can also entrap the lingual nerve producing the odd symptom of a bitter, metallic taste in the mouth (which the patient may not connect with other symptoms and may not report for fear of being thought "crazy.")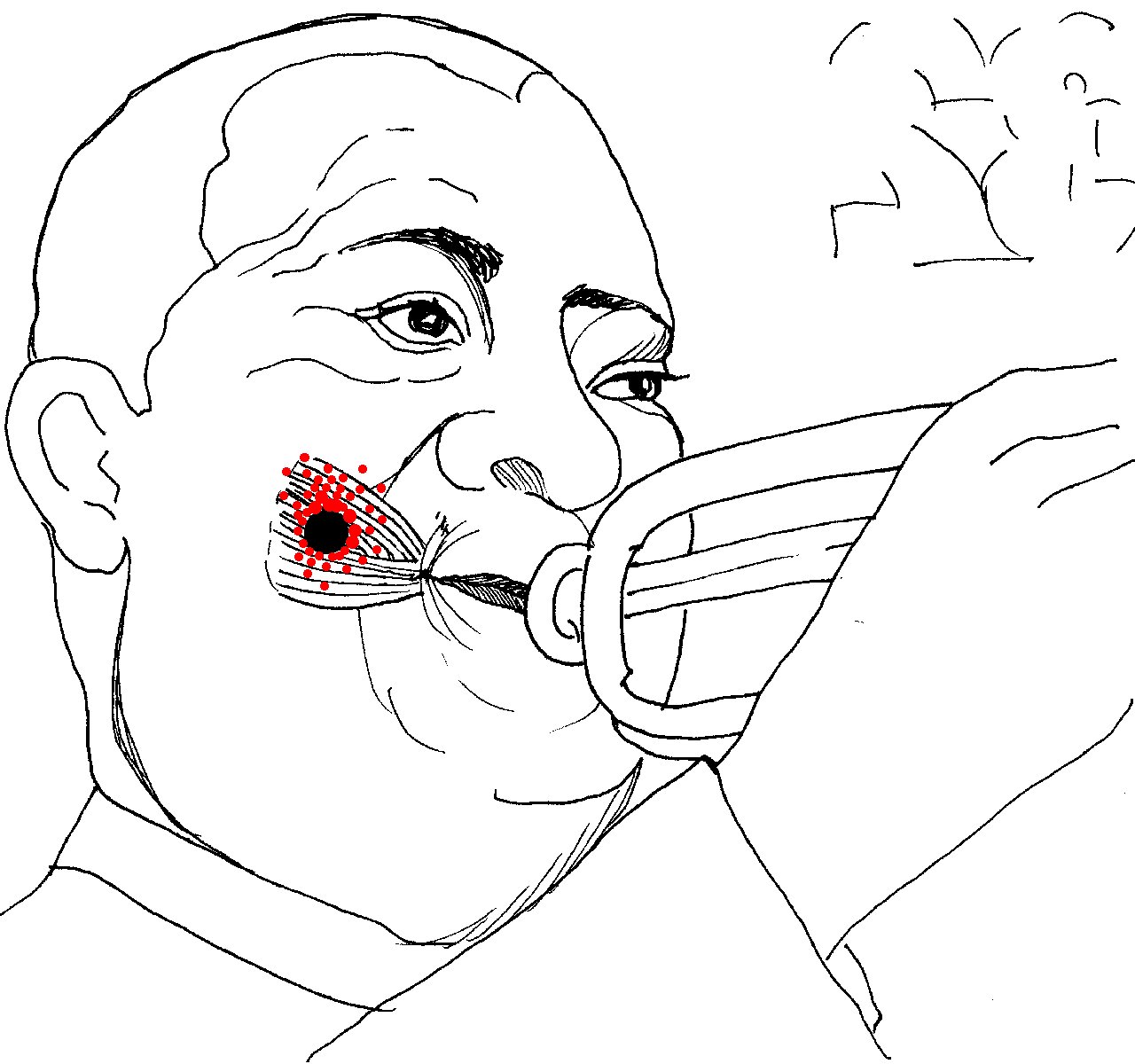 the part of the cheek that puffs out when playing the trumpet (for which it is named), blowing up balloons or stuffing one's mouth too full. Buccinator pain may appear suddenly following dental/orthotic work. There are no entrapments by the buccinator itself, but the lateral pterygoid can entrap the buccal nerve which supplies the skin and mucous membrane in this area. The muscle itself can cause local pain deep in the cheek while chewing, commonly misdiagnosed as TMJ dysfunction.
the part of the cheek that puffs out when playing the trumpet (for which it is named), blowing up balloons or stuffing one's mouth too full. Buccinator pain may appear suddenly following dental/orthotic work. There are no entrapments by the buccinator itself, but the lateral pterygoid can entrap the buccal nerve which supplies the skin and mucous membrane in this area. The muscle itself can cause local pain deep in the cheek while chewing, commonly misdiagnosed as TMJ dysfunction.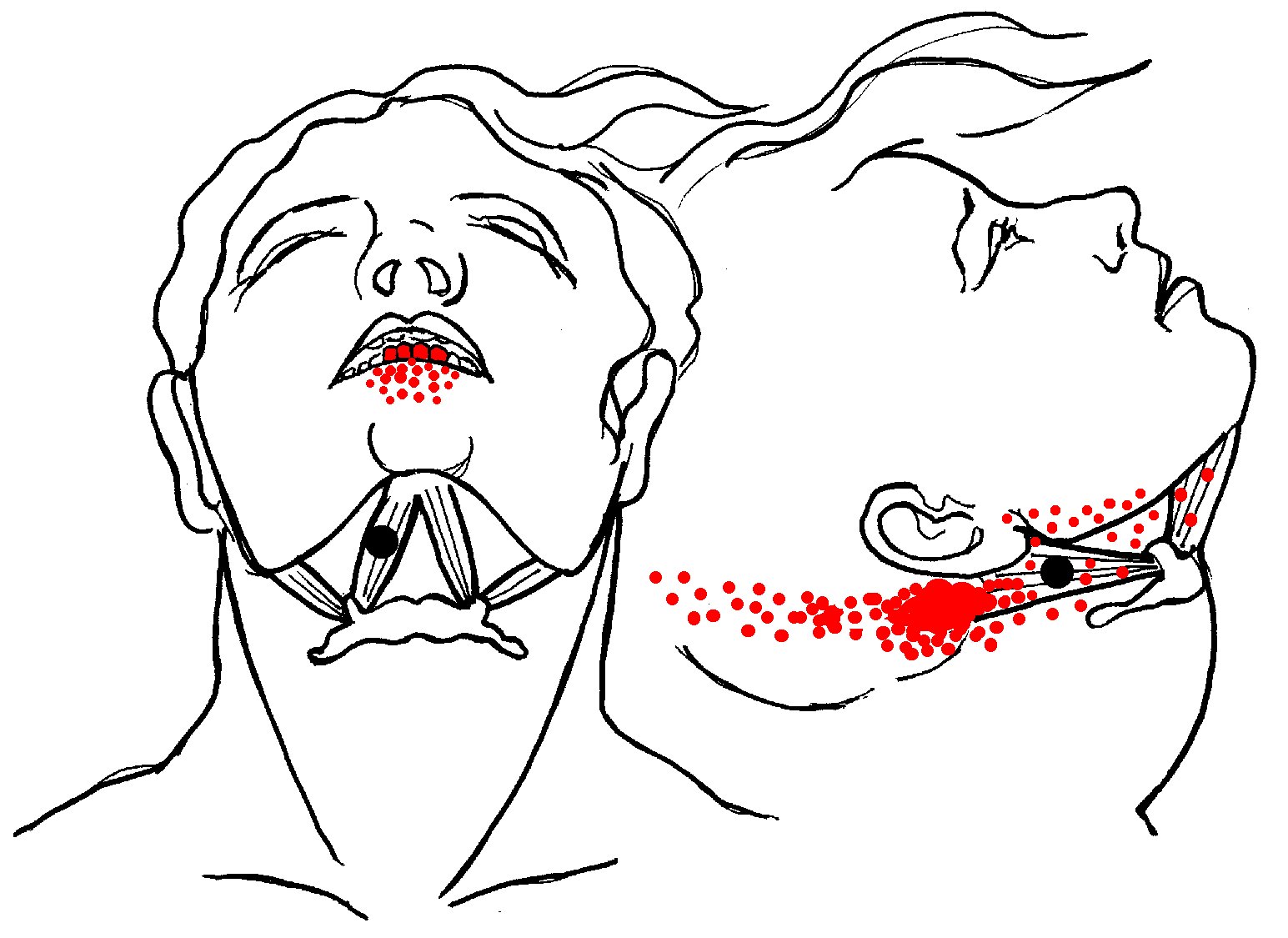 Strained by retrusion of the jaw (as in playing the clarinet or similar wind instruments) or by holding a violin in place with the chin. Commonly damaged in whiplash injuries in concert with other neck muscles such as trapezius and splenius. Trigger points in the anterior belly send pain to the four lower incisor teeth and the alveolar ridge. There may also be pain in the throat and tongue and difficulty swallowing because of the relationship to the hyoid bone.
Strained by retrusion of the jaw (as in playing the clarinet or similar wind instruments) or by holding a violin in place with the chin. Commonly damaged in whiplash injuries in concert with other neck muscles such as trapezius and splenius. Trigger points in the anterior belly send pain to the four lower incisor teeth and the alveolar ridge. There may also be pain in the throat and tongue and difficulty swallowing because of the relationship to the hyoid bone.Trigger points in the posterior belly refer pain to the upper sternocleidomastoid muscle, pain to the throat possibly as far back as the occiput. There may also be difficulty swallowing and a bothersome feeling of a persistant "lump" in the throat. That "lump" may be the hyoid bone which, again, is not moving properly.
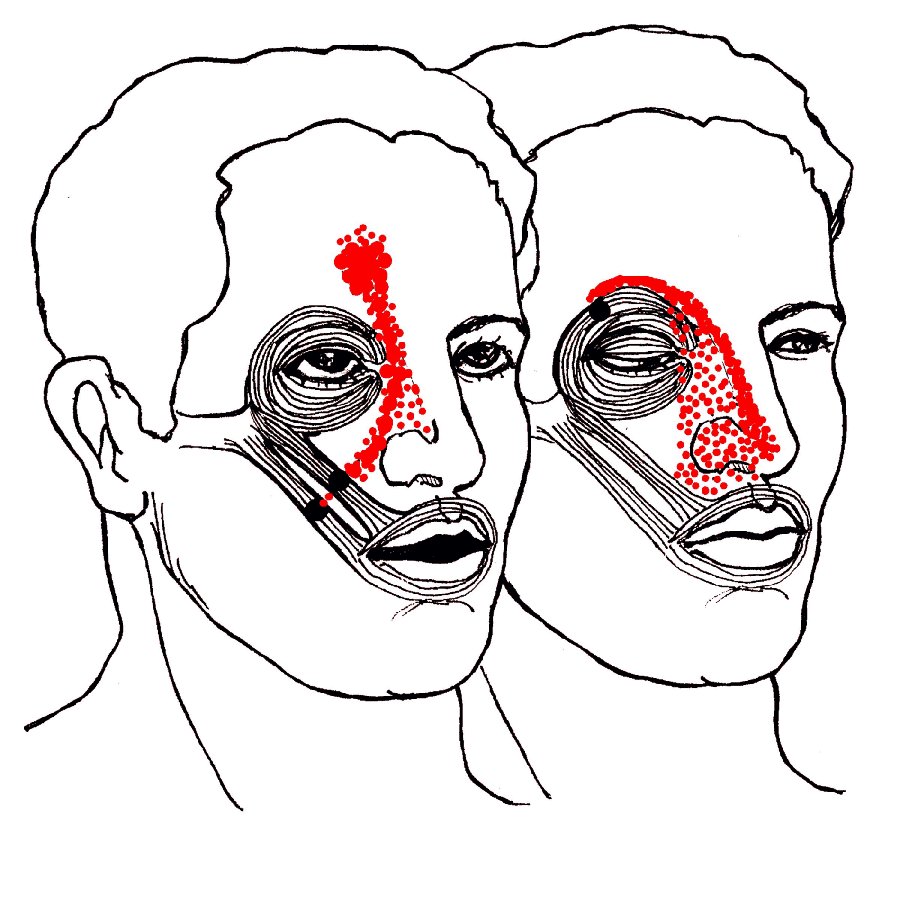
Orbicularis and zygomaticus are the only two muscles that refer pain to the nose. Both patterns are commonly mistaken for "sinus" pain but may be due to a blow to the eye or simply smiling too long at the reception.
Zygomaticus can entrap blood vessels that travel from cheek to nose and up to the forehead. The resulting pain is not "sinus," it's a muscle cramp due to reduced blood and oxygen supply -- but no less painful.
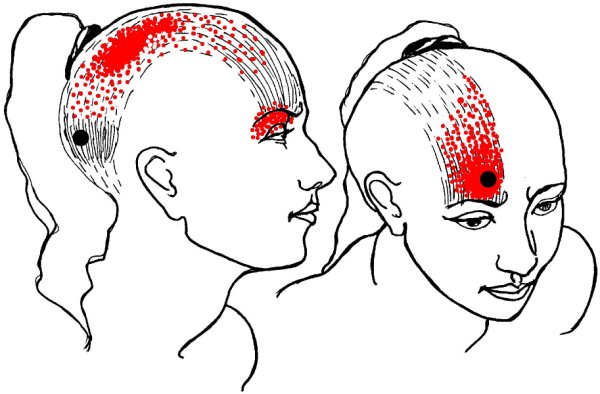
Trauma to the scalp fascia or the occipitalis at the back of the skull can transmit pain through the head and into the eye. Trauma may include a blow to the back of the head, strain from a tight ponytail or bun, or the weight of long, heavy hair. In one case I know of, a man struck the top of his head on the corner of a cabinet. Result: a slight puncture wound in the scalp, a brutal pain in the eye.
Frontalis helps open the eyes, raises the eyebrows, and wrinkles the forehead into "worry lines." It is commonly used by biofeedback practitioners to monitor muscle tension. Trauma to frontalis (whether a blow to the forehead or habitual frowning) can cause severe frontal headache often diagnosed as "migraine." Frontalis is one of the muscles that definitively proved the muscle-migraine connection.
Botox injections paralyzed the frontalis, eliminating "worry lines" but they also had the surprising side effect of halting chronic "migraines". Or maybe not so surprising, as frontalis entraps the supraorbital nerve. The related corrugator supercilii (at the top of the nose between the eyebrows) compresses branches of the supraorbital nerve along with the supratrochlear nerve and branches of the supraorbital nerve. All of these are branches of the trigeminal nerve which is heavily involved in migraine. You can treat trigger points with great results -- or, avoid compressing those muscles. Your frown may be giving you a headache!
Semispinalis capitis is commonly injured in auto accidents. You can injure it more slowly but just as effectively with a chronic head-forward position.
When tight, semispinalis may entrap the greater occipital nerve which in turn causes numbness, tingling and/or burning pain extending over the back of the head to the top (vertex) of the head. It may be difficult to touch chin to chest, and sufferers may be unable to bear the pain of laying the back of the head on a pillow.
Relieve nerve pain with cold.
Relieve muscle pain with moist heat.
In either case, look for the origin of the pain, rarely the spot where it hurts.
This muscle typically produces a vague band of pain from occiput along side of head to just behind orbit (similar to suboccipital pain pattern).
This pain arises from the tiny muscles that run between the individual vertebrae of the spine.
This muscle is the Number One cause of "stiff" or "wry" neck and the second most common shoulder girdle muscle (trapezius is Number One) to have trigger points. Working with trapezius, levator shrugs the shoulders and helps prevent forward flexion of the neck, hence it is also damaged in whiplash injuries. In daily life, it is commonly strained when shoulder (or shoulders) are chronically hunched, either in stress, or by attempting to keep a strap from sliding off the shoulder, especially when the muscle is cold or fatigued. Pain in the angle of the neck and along the vertebral border of the scapula may be so severe that patient cannot move the neck at all.
 The four pairs of suboccipital muscles cause deep aching pain running in a band from the back of the head to the orbit of the eye, possibly with balance problems and dizziness. One of these (the rectus capitis superior minor) attaches directly to the dura mater of the spinal cord. When traumatized it can produce odd visual and neurological symptoms to the point of seizures.
The four pairs of suboccipital muscles cause deep aching pain running in a band from the back of the head to the orbit of the eye, possibly with balance problems and dizziness. One of these (the rectus capitis superior minor) attaches directly to the dura mater of the spinal cord. When traumatized it can produce odd visual and neurological symptoms to the point of seizures.Suboccipitals are commonly strained or hypertrophied in persons who wear bifocals, children who watch TV lying with chin propped on hands, and anyone who habitually holds the head in position with chin up and neck flexed backward.
 Pain from this muscle also appears in the sacrum at the sacro-iliac joint and then reappears in the face and jaw where it may fire off symptoms of TMJ and toothache. "But," you say, "migraine is vascular!"
Pain from this muscle also appears in the sacrum at the sacro-iliac joint and then reappears in the face and jaw where it may fire off symptoms of TMJ and toothache. "But," you say, "migraine is vascular!"Indeed it is -- and the soleus is the other end of the cardio-vascular system. It is known as "The Second Heart" because its pumping action returns blood from the lower extremities to the heart. I have stopped many full-blown migraines by working adductor and calf muscles.
"But," you say, "migraine is neurological!"
Indeed it is -- and tightness and restriction in soleus and the adductor magnus can cause serious impingement of neurovascular structures including the femoral nerve, femoral artery, and femoral vein (at the adductor hiatus of the adductor magnus) and the posterior tibial nerve, vein, and artery by the soleus. (The plantaris, a slip of the soleus muscle, can also entrap the popliteal artery at the back of the knee.) Entrapment by these muscles can be so severe that the patient may lose deep tendon reflexes. Short of that, it's no surprise that a sufferer might have cold feet.
Upstream, entrapment by the adductors can be brought on by failing to stretch out after using the thigh machines at the gym and very commonly, by footwear. It may be difficult to believe that shoes (whether you call them "cowboy boots" or "high heels") may be causing your jaw and head pain, but it is often true. Knee-high stockings with tight, constricting bands will do the job and I have also seen a man who never had headaches in his life until he caught some shrapnel in the calf. Even worse can happen, however.
When the soleus can no longer work as "the second heart" due to inactivity or constriction, there can be side effects far worse than migraine. Pooling and subsequent clotting of blood in the lower extremities is involved in deep vein thrombosis, also known as "airline thrombosis" due to the consequences of a cramped seat and long periods of inactivity. The condition is very real, but sadly mis-named. The condition arises far more commonly from long hours of sitting at a desk than from (relatively rare) airline travel.
