|

WELCOME..."LIFE...AND THE THINGS IT BRINGS" SOMETIMES, OUR LIVES CAN BE TURNED UPSIDE DOWN AND IT IS UP TO US & THE CHOICES, WE MAKE...THAT WILL DETERMINES THE OUTCOME. HOW WE HANDLE IT IS IMPORTANT, FOR THE CHOICES WE MAKE..DO MAKE A DIFFERENCE. LIFE,IS WHAT WE MAKE IT. SO,LET US ALL MAKE LIFE GOOD. ALWAYS "PAY IT FORWARD". WE CAN DO IT. :) DO TO OTHERS, AS YOU WOULD HAVE DONE TO YOU. GOD BLESS..
"MY MOTTO"
LIFE...AND THE THINGS IT BRINGS
Tuesday, December 27, 2011
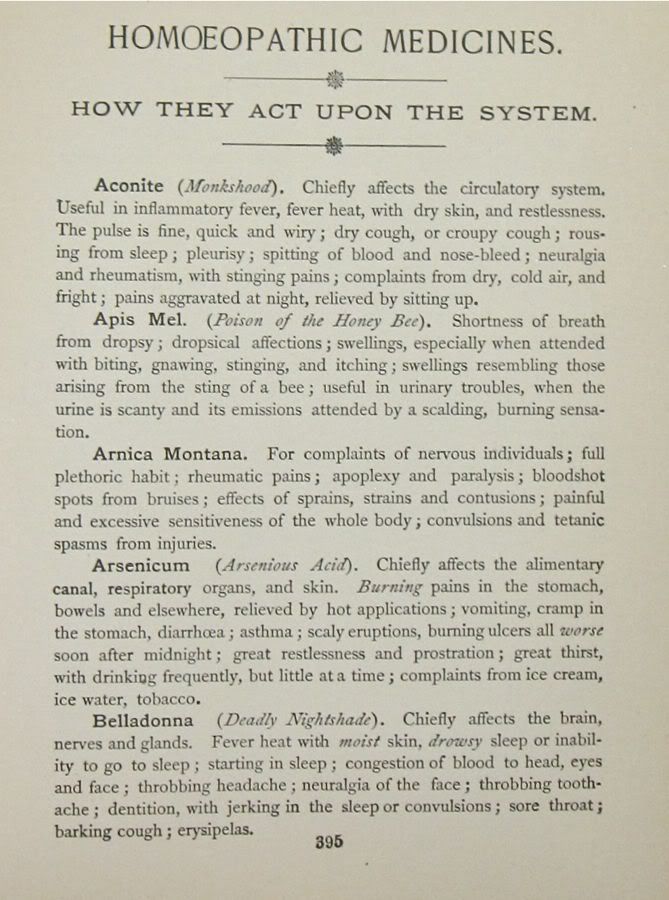
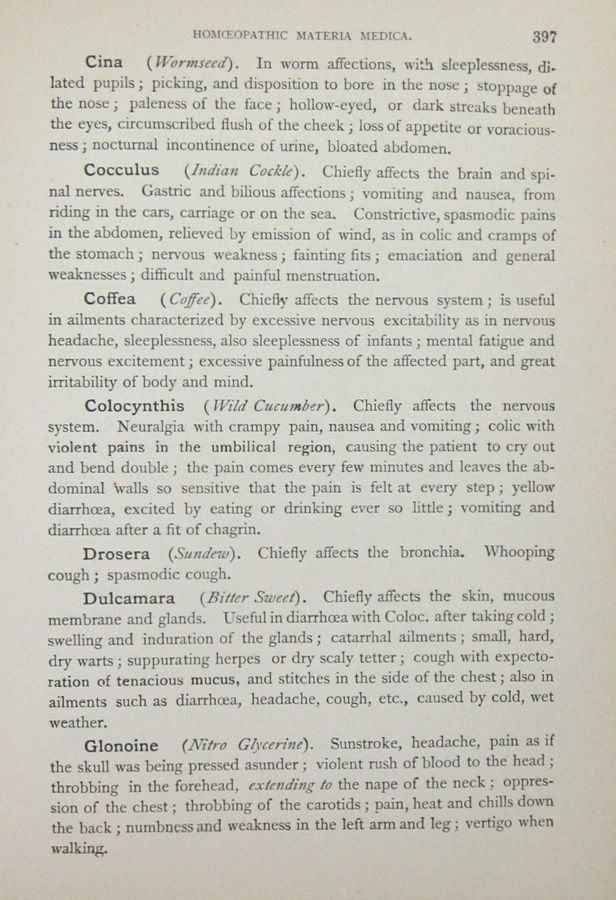
ALLOPATHY & HOMEOPATHY

Sunday, November 6, 2011
I THINK I AM GOING TO TRY TRADITIONAL CHINESE MEDICINE INSTEAD OF THE ROUTE I HAVE BEEN GOING
I AM SO TIRED GUYS AND I HAVE BEEN DOWN FOR SUCH A LONG TIME AND I AM SO WEIRY, BECAUSE I HAVEN'T FOUND THE ANSWER TO WHAT HAS BEEN KEEPING ME DOWN. UNFORTUNATELY, I LI VE IN THIS BED AND DREAM OF A DAY WHEN MY LIFE TURNS BACK AROUND AND I START LIVING AGAIN.
I DON'T WANT TO LIVE HERE THE REST OF MY LIFE. I KNOW, IT IS HARD FOR ANYONE THAT DOESN'T EXPERIENCE THIS "NIGHTMARE", TO UNDERSTAND. IT IS UTTERLY IMPOSSIBLE FOR THAT TO HAPPEN, UNLESS U TRULY KNOW WHAT PAIN AND DISPAIR IS AND ARE OR HAVE FELT IT IN UR LIFE.
 I MUST SAY, I ONCE HAD A LIFE THAT WAS FULL AND BUSY. I LOVE TO WORK AND BE AROUND PEOPLE AND I LIKED THAT KIND OF LIFE. IT WAS A LIFE TO WHERE, WHEN U WAKE UP IN THE MORNING, U CAN PLAN UR DAY AND DO WHATEVER IT IS THAT NEEDED TO BE DONE.
I MUST SAY, I ONCE HAD A LIFE THAT WAS FULL AND BUSY. I LOVE TO WORK AND BE AROUND PEOPLE AND I LIKED THAT KIND OF LIFE. IT WAS A LIFE TO WHERE, WHEN U WAKE UP IN THE MORNING, U CAN PLAN UR DAY AND DO WHATEVER IT IS THAT NEEDED TO BE DONE.
THAT IS DEFINITELY NOT MY LIFE NOW...NO, I LAY HERE AND SUFFER MOST OF THE TIME, BUT I DO THINK @ WHAT LIFE I HAVE HAD AND WAS BLESSED WITH. I COULD GO AND DO ANYTHING THAT I WANTED AND FELT SO ALIVE AND WELL, BUT NO NOW. NO, I DREAM A LOT AND THINK @ HOW MY LIFE USED TO BE AND I AM GREATFUL THAT I DID AT LEAST, GET TO EXPERIENCE WHAT I HAVE IN MY LIFE
I GOT TO SING AND GIVE MY MUSIC TO EVERYONE AND TO ME, IT WAS LIVING.:))
I AM GREATFUL GOD 4 THE LIFE YOU HAVE BLESSED ME WITH AND I THANK YOU 4 IT. I TRULY HAVE HAD A WONDERFUL LIFE, BUT IT SURE CHANGED ON ME SO FAST.
PLEASE LORD, GIVE ME SOME OF MY LIFE BACK. HELP ME TO BE THE MOM THAT I NEED TO BE. I KNOW THEY HAVE DONE WITHOUT ME, MANY TIMES AND WANTED ME TO BE THERE, BUT I COULDN'T. I WASN'T ABLE...GOD KNOWS, IT IS TRUE.
IF THERE WAS ANYTHING I COULD'VE DONE TO BE THERE, I WOULD DO, BUT UNFORTUNATELY...MOM WASN'T ABLE AND THAT IS THE GODS HONEST TRUTH.
IF I HAD A CHOICE IN THE MATTER I WOULD ALWAYS MAKE EACH AND EVERY FUNCTION OR IMPORTANT TIME THAT U WANTED ME TO BE THERE. IT HAS HURT ME SO MUCH...MORE THAN U KNOW TO NOT HAVE BEEN ABLE OR CAPABLE TO BE THERE AND I AM SORRY TO THE BOTTOM OF MY HEART. IT HAS TO BE ONE OF THE HARDEST THINGS FOR A MOM TO HAVE TO DO...BE AWAY FROM MY SONS.
 I KNOW, THEY HAVE MISSED ME, ON MORE THAN ONE OCASION AND I AM TRULY SORRY. MOM IS TELLING THE TRUTH. AS BAD AS I HATE TO SAY IT...I AM REALLY SICK AND IT SEEMS THAT NO ONE IS TAKING ME SERIOUSLY. WHY IS IT SO HARD FOR PEOPLE TO SEE JUST SICK I AM? I CAN'T STAND ON MY OWN TWO FEET FOR 5 MINUTES, B4 I START FEELING MY BACK START TO BURN. IT STARTS IN MY RIBS AND IT WILL COVER MY BACK. I AM TALKING @ A SHEET OF FIRE AND I HAVE TO FIND SOMEWHERE TO LEAN BACK STRAIGHT ON (that is the only thing that will give me a minute b4 I have to get to the bed and fast)OR IT WILL GET SO BAD THAT THE PAIN IS SO EXCRUCIATING AND IT IS HORRIBLE.:((
I AM SCARED, AT TIMES. ESPECIALLY, AT MOMENTS, BUT THE LORD IS THERE...HE IS WITH ME AND HE COMFORTS ME.:))) IF IT HADN'T BEEN 4 HIM, I DON'T THINK...NO, I KNOW , I WOULDN'T BE HERE. SO, I THANK HIM 4 ME SURVIVING THIS FAR AND I KNOW THAT SOUNDS REALLY MORBID, BUT U JUST DON'T KNOW THE TIMES I EXPERIENCE. IT IS MISERY WHEN I HAVE THE "EPISODES". I CALL THEM THAT BECAUSE IT IS SO SCARY THAT IT IS AN EPISODE. I WILL GET TO FEELING MY SKIN TIGHTEN UP ALL OVER..LIKE, I AM SUFFICATING IN A WAY OR MY BODY IS. IT FEELS LIKE IT CAN'T GIVE ANYMORE, THEN MY HEART WILL BEAT SO HARD IN MY CHEST...THEN, THIS IS THE KICKER...MY FACE WILL GET COMPLETELY NUMB, WITH PIN/NEEDLE FEELING(same feeling, as when u foot goes numb and how it feels when u stomp on it. It is the same feeling u get after the Dentist has given u a few shots of NOVACANE in ur jaw).
I KNOW, THEY HAVE MISSED ME, ON MORE THAN ONE OCASION AND I AM TRULY SORRY. MOM IS TELLING THE TRUTH. AS BAD AS I HATE TO SAY IT...I AM REALLY SICK AND IT SEEMS THAT NO ONE IS TAKING ME SERIOUSLY. WHY IS IT SO HARD FOR PEOPLE TO SEE JUST SICK I AM? I CAN'T STAND ON MY OWN TWO FEET FOR 5 MINUTES, B4 I START FEELING MY BACK START TO BURN. IT STARTS IN MY RIBS AND IT WILL COVER MY BACK. I AM TALKING @ A SHEET OF FIRE AND I HAVE TO FIND SOMEWHERE TO LEAN BACK STRAIGHT ON (that is the only thing that will give me a minute b4 I have to get to the bed and fast)OR IT WILL GET SO BAD THAT THE PAIN IS SO EXCRUCIATING AND IT IS HORRIBLE.:((
I AM SCARED, AT TIMES. ESPECIALLY, AT MOMENTS, BUT THE LORD IS THERE...HE IS WITH ME AND HE COMFORTS ME.:))) IF IT HADN'T BEEN 4 HIM, I DON'T THINK...NO, I KNOW , I WOULDN'T BE HERE. SO, I THANK HIM 4 ME SURVIVING THIS FAR AND I KNOW THAT SOUNDS REALLY MORBID, BUT U JUST DON'T KNOW THE TIMES I EXPERIENCE. IT IS MISERY WHEN I HAVE THE "EPISODES". I CALL THEM THAT BECAUSE IT IS SO SCARY THAT IT IS AN EPISODE. I WILL GET TO FEELING MY SKIN TIGHTEN UP ALL OVER..LIKE, I AM SUFFICATING IN A WAY OR MY BODY IS. IT FEELS LIKE IT CAN'T GIVE ANYMORE, THEN MY HEART WILL BEAT SO HARD IN MY CHEST...THEN, THIS IS THE KICKER...MY FACE WILL GET COMPLETELY NUMB, WITH PIN/NEEDLE FEELING(same feeling, as when u foot goes numb and how it feels when u stomp on it. It is the same feeling u get after the Dentist has given u a few shots of NOVACANE in ur jaw).
I MUST SAY THIS IS ONE OF CREEPIEST, SCARRIEST FEELINGS A PERSON CAN ECER HAVE. IT FEELS LIKE UR HAVING A STROKE. NOW, ONE TIME,WHILE ALL THIS WAS HAPPENING...THE WHOLE LEFT SIDE OF MY BODY WENT COMPLETELY LIMP. I COULDN'T MOVE, AT ALL. I HAD TO CALL 911, BECAUSE I COULDN'T MOVE THE WHOLE LEFT SIDE OF MY BODY, AT ALL. IT WAS PARALYSED COMPLETELY. I FELT LIKE A 40LB. WEIGHT WAS LAYING ON MY LEFT ARM AND LEG. I THOUGHT FOR SURE THAT I WAS HAVING A STROKE. WHAT ELSE COULD IT BE?..A HEART ATTACK, MAYBE, I DONNO I AM THE ONE WHOS BRAIN IS NUMB..LITERALLY AND SCARED OUT OF MY MIND THINKING...WELL, THIS IS IT.
WOULDN'T U WANT TO KNOW WHAT CAUSED UR BODY TO GO COMPLETELY NUMB AND TO DO THIS?...WHY OF COURSE U WOULD. GUYS, I AM JUST TIRED AND KNOW THERE IS SOMEONE WRONG AND IT HAS GOT TO BE FOUND. THERE IS SOMEONE OUT THERE THAT HELP ME..SURELY THERE IS SOMEONE THAT CAN FIX ME.
I THINK, I MADE THE MISTAKE OF THINKING A NEUROLOGIST WAS THE ANSWER TO WHAT I HAVE, I GUESS. NOW, I AM LEANING TOWARD SEEING AN ENDOCRINOLOGIST, AN ONCOLOGIST AND AN INFECTIOUS DISEASE DOC. I ONLY THINK THAT SINCE I HAVE A LOT OF PROBLEMS WITH MY BLOOD THAT IS WHERE I SHOULD START, BUT IN THE MEANTIME, IT WON'T HURT ME TO CHECK OUT THE TCM. IT MIGHT HELP ME, SO IT IS WORHT A TRY.:)
THIS TRADITIONAL CHINESE MEDICINE. IT IS ALL NATURAL AND MAYBE WHAT MY BODY NEEDS. IT IS WORTH A TRY. I HAVE HEARD SO MANY EXCELLENT OUTCOMES FROM IT. I AM JUST READY TO GET THIS SITUATION TO CHANGE. IT HAS TO, SOMEWAY.
I KNOW THAT THIS HAS GONE ON FOR TOO LONG (it started in '03, with just a neck pain and i couldn't sleep and wound up with surgery that took my C5-C6 out) I JUST KNOW THAT THIS IS RIDICULAS THAT THE DOCS CAN'T GIVE ME AN ANSWER.
AGAIN, I HAVE ONLY BEEN GOING TO SEE NEUROLOGISTS, ALL THIS TIME AND THINK THAT THIS WAS MY FIRST MISTAKE. I SHOULD'VE GONE TO SEE SOME OTHER KINDS OF DOCTORS...I SEE THAT NOW, BUT, I WAS HURTING IN MY NECK AND FELT IT WAS SOME KIND OF MECHANICAL PROBLEM THAT HAS GONE WRONG WITH THE TITANIUM PLATES OR THE SCREWS THAT HELD THEM IN PLACE.
 I CAN'T IMAGINE WHAT PEOPLE ARE WONDERING. I CAN SEE ALL SORTS OF THE WRONG THING S CIRCULATING OUT THERE AND WHEN...HERE, I LAY HELPLESS AND SOMETIMES FEEL HOPELESSTHAT I WILL NEVER BE ME AGAIN. I AM IN DEBILITATING PAIN THAT I JUST WANT TO END..SOMEWAY. ALL I WANT IS MY LIFE BACK.
I CAN'T IMAGINE WHAT PEOPLE ARE WONDERING. I CAN SEE ALL SORTS OF THE WRONG THING S CIRCULATING OUT THERE AND WHEN...HERE, I LAY HELPLESS AND SOMETIMES FEEL HOPELESSTHAT I WILL NEVER BE ME AGAIN. I AM IN DEBILITATING PAIN THAT I JUST WANT TO END..SOMEWAY. ALL I WANT IS MY LIFE BACK.
THE PICTURE ABOVE, SHOWS THE SWELLING IN MY FACE(moon face) AND MY OVERALL BODY WEIGHT GOT UP TO 199...WOW, I WAS FAT AND MISERABLE. NOW, AT LEAST, I AM BACK DOWN TO 145 AND THAT IS SOMETHING, BUT THE PAIN IS STILL THERE.
I DON'T KNOW WHAT HAS ME, I JUST KNOW THAT I AM LIVING BASICALLY A "HELL ON EARTH" SCENERIO ,RIGHT NOW. (forgive me Lord..don't mean that disrespectfully in any way) BECAUSE, ANYWAY THAT U LOOK AT IT, I AM STILL BLESSED.:))<3
I DO KNOW GOD HAS A REASON 4 EVERYTHING AND AS LONG AS HE IS IN CONTROL, I WILL ACCEPT WHAT MY LIFE IS BECAUSE I KNOW GOD IS IN CONTROL. I WILL ALSO CONTINUE TO FIGHT TO FIND THE ANSWERS AND TRY TO GET MY LIFE BACK... AND WHO WOULDN'T?
WE ARE SUPPOSE TO STRIVE TO LIVE A GOOD LIFE AND TO LIVE IT FOR THE LORD. HE GAVE US EVERYTHING...HE EVEN GAVE US HIS LIFE AND I KNOW THAT I AM GREATFUL. I WAS BLESSED WITH TWO WONDERFUL PARENTS, THAT LOVE AND TAKE GOOD CARE OF ME. MOM COOKS ALL THE TIME AND SHE IS NOT WELL. I WORRY @ HER AND WHAT SHE TRIES TO DO FOR ME. SHE PUSHES HERSELF SO HARD, BUT I CAN SEE IT. I CAN SEE THAT SHE ISN'T WELL. AFTER ALL, SHE DOES HAVE A CYST ON HER LIVER. AND DAD RUNS ALL THE TIME DRIVING ME HERE AND THERE...IF, I CAN GO THAT IS AND HAVE A DAY TO WHRE, I CAN AT LEAST, GET READY TO GO.

 I NEED TO GET WELL, SO I CAN TAKE CARE OF THEM FOR A CHANGE. I PRAY THAT IS SOON, LORD. I WANT AND NEED TO BE ABLE TO SPEND MORE TIME LAUGHING, FISHING, EATING, SINGING AND LOVING AND LIVING MY LIFE...BUT, THIS TIME LORD...U WILL BE RIGHT THERE BESIDE ME, ALL THE WAY.:)))<3
I NEED TO GET WELL, SO I CAN TAKE CARE OF THEM FOR A CHANGE. I PRAY THAT IS SOON, LORD. I WANT AND NEED TO BE ABLE TO SPEND MORE TIME LAUGHING, FISHING, EATING, SINGING AND LOVING AND LIVING MY LIFE...BUT, THIS TIME LORD...U WILL BE RIGHT THERE BESIDE ME, ALL THE WAY.:)))<3
REGARDLESS OF MY PAIN, I DO HAVE A GOOD LIFE, BUT MAYBE THIS IS A LESSON THAT I NEEDED TO LEARN. I DO KNOW THAT I REALLY HAVE BEEN HUMBLED, SINCE I GOT SICK. IT HAS CHANGED MY LIFE...ONLY 4 THE BETTER, BECAUSE I KNOW GOD AND THAT IS MORE IMPORTANT THAN ANYTHING, IN THE WORLD. I AM SO GLAD, I AM HIS.:D
I AM GLAD THAT I FOUND HIM...AND THAT HE FOUND ME.:)))
DEAR LORD, U KNOW WHAT I AM GOING THROUGH AND I PRAY THAT MY LIFE IS GOING TO CHANGE, IF IT IS UR WILL...TO WHERE I CAN JUST WALK AROUND AND BE HAPPY AGAIN. I PRAY 4 MY FAMILY TO GET THROUGH THIS AND TO UNDERSTAND IT ALL. I REALLY BELIEVE THAT SOMETHING IS SEIOUSLY WRONG WITH ME AND I HOPE THAT IT DOESN'T TAKE ME AWAY FROM HERE JUST YET. IF IT IS "UR WILL LORD". I JUST WOULD LOVE TO ENJOY MY FAMILY AND DO THINGS WITH THEM AGAIN. I JUST MISSED OUT ON SO MUCH AND SO MANY THINGS WITH MY FAMILY I WANT TO MAKE THAT UP, IF I CAN. I REALLY NEED AN ADVOCATE, LORD..TO FIGHT TO GET ME WELL.
DEAR LORD, SEND ME AN ADVOCATE BECAUSE MY MOM AND DAD DON'T KNOW WHAT TO DO TO FIND OUT WHAT IS WRONG WITH MEAND I KNOW THEY ARE SO TIRED. MY HUSBAND, WORKS ALL THE TIME AND THAT MAKES IT HARD TO DEDICATE ANY TIME, TO TRAVEL AND GO TO DOCS.
LORD, EVERYDAY I BATTLE THIS PAIN AND I PRAY THAT I WILL GET WELL. I DO ALSO PRAY THAT NO ONE HAS TO FEEL THIS PAIN, IF I MAY BECAUSE IT IS SO BAD. ...AND I JUST WANT IT TO BE OVER. I KNOW, LORD...YOU HAVE KEPT ME HERE AND I AM THANKFUL 4 THAT. :D
PLEASE ANSWER MY PRAYER LORD AND GET ME WELL.:)<3

WELL, I MUST SAY THAT I HAVE REALLY TRIED TO SEE IF THE WESTERN MEDICINE COULD HELP ME, BUT I AM NOT GETTING ANY BETTER. I AM STILL IN PAIN AND AS A MATTER OF FACT, I AM GETTING WORSE(sad 2 say). SO, I HAVE TO DO SOMETHING TO GET WELL BECAUSE THIS PAIN IS EVERYDAY, ACTUALLY FEELS LIKE IT COULD KILL ME SOMETIMES, BUT I KEEP MOVING ON...AND IT DOES GET VERY VERY OLD TO DEAL WITH.
ALSO, I DO KNOW THAT IT MUST BE HARD ON THE ONES I LOVE AND THAT LOVES ME. I CAN ONLY IMAGINE IT BEING ONE OF MY KIDS. MY HEART WOULD BE BROKEN. I WOULDN'T WANT TO SEE THEM LIKE THAT. SO, I KNOW MY MOM AND DAD HAVE REALLY WORRIED @ ME AND HAVE BEEN THROUGH IT. SO MANY TIMES HAVE THEY GOT UP EARLY IN THE MORNING TO DRIVE ME TO ANOTHER DOC OR HAD TO SIT AND WATCH ME SCREAM OUT IN PAIN. IT MAKES ME SAD THAT THEY ARE HAVING TO GO THROUGH THAT, BUT I DON'T KNOW WHAT TO DO THAT COULD MAKE IT ANY EASIER ON THEM??;(
I AM THE ONE SUFFERING HERE AND IT IS HARD, WHEN SOMETHING SO PAINFUL HAS A HOLD OF U AND IT DOESN'T JUST STOP OR LET UP...NO, IT EASES UP SOME AND I CAN BREATH WITH SOME ~SIGH~ OF RELIEF...UNTIL, IT COMES BACK.
IT IS HORRIBLE AND SO DEBILITATING AND EXCRUCIATING AT TIMES, I FEEL LIKE I AM HAVING A STROKE OR SOMETHING,FOR THE WHOLE LEFT SIDE OF MY BODY GOES COMPLETELY NUMB AND IT HAS GONE COMPLETELY PARALYZED ON MY LEFT SIDE. THAT IS BAD.
THIS CAN BE A SIGN OF "MS", BUT I HAVEN'T BEEN DIAGNOSED WITH THAT AND AM GLAD, BUT AND YES, THERE IS A BUT IN THERE. THE DOCS DID FIND A LESION ON MY THORACIC AND THE THE NEUROLOGIST THAT FOUND IT SAID THAT IT WAS OUT OF HIS AREA OF EXPERTISE AND JUST LEFT ME HANGING WITH NO ONE TO GO TO OR SEE. I JUST WANT TO SEE SOMEONE THAT HAS EXPERTISE, BUT WHERE ARE THEY? IT IS HARD TO FIND A DECENT DOC THAT WON'T TREAT U LIKE A SWINGING DOOR..."NEXT". I HOPE THAT I DON'T HAVE MS AND THEY HAVEN'T SAID I HAVE THAT YET AND I AM PRAYING THAT I DON'T.
I DO KNOW THAT SOMETHING IS TERRIBLY WRONG, BUT I AM NOT A DOCTOR. ALL I CAN DO IS RESEARCH AND BE INFORMED OF THE POSSIBILITIES. I NEVER TRY TO DIAGNOSE MYSELF, I ONLY COMPARE ALL OF THE SYMPTOMS OF SOMETHING AND THEN, I WRITE THAT DOWN AND COMPARE FROM THE LIST. I THEN, TAKE MY THEORIES TO THE DOC TO SEE, IF THEY SAY IT IS A POSSIBILITY OR NOT. THERE IS SO MANY DIFFERENT POSSIBILITIES OF WHAT IT COULD BE. WE HAVE TO BASICALLY BE OUR OWN BE ADVOCATES SOMETIMES, BUT I AM TIRED AND NEED HELP.
NO, I CAN'T DIAGNOSE MYSELF, NO ONE CAN AND IT MUST SEEM THAT WAY BECAUSE, I POST SO MANY DIFFERENT ARTICLES AND @ MANY DIFFERENT THINGS. THE ONLY REASON I DO IS BECAUSE I FIND IT INTERESTINGLY ENOUGH, TO SAVE IT AS A SORT OF DOCUMENTATION OF WHAT I AM GOING THROUGH AND ALSO, TO SHARE IT WITH OTHERS. I KNOW, THERE COULD BE OTHERS THAT COULD HAVE A PARTICULAR INTEREST, IN SAID SUCH ARTICLE, SO I POST IT FOR ALL.
I DO THINK OF OTHERS AND TO ME...MY MOTTO WOULD BE, "I WOULD RATHER BE INFORMED, THAN UNINFORMED"...ESPECIALLY, WHEN IT COMES TO OUR HEALTH. THESE DAYS, IT IS WAY TOO IMPORTANT TO TRY TO STAY AS HEALTHY AS WE CAN.
I HAVE BEEN GOING TO DOCS AND TELLING THEM WHAT I FEEL AND WHAT I GO THROUGH AND THEY HAVE MADE DIANOSIS'S AND PRESCRIBED THERAPY, MEDICINES AND RUN MANY TESTS, BUT THEY HAVEN'T FOUND THE ELUSIVE ONE YET...NO, NOT THE ONE THAT IS KEEPING ME IN THIS BED!
I AM SO TIRED OF SEEING DOCTORS THAT ARE NOT FINDING THE ANSWER TO WHAT IT IS THAT IS MAKING ME SICK AND IN SO MUCH PAIN. SO, THAT IS WHY I AM LOOKING FOR SOMEONE THAT PRACTICES TCM. I FEEL IF IT CAN CURE SOME CANCERS, IT POSSIBLY COULD CURE ME.
ONE MORE WORD OR TWO B4 I GO. I DO KNOW THAT IT IS HARD TO UNDERSTAND WHAT SOMEONE IS GOING THROUGH AND NOT MANY PEOPLE CAN RELATE TO SOMEONE ELSE'S PAIN, NOT TOTALLY. I AM IN CHRONIC PAIN AND I AM SO TIRED.
I MUST FIND AN ANSWER TO WHAT IS TAKING MY LIFE AND THROWING IT ALL AWAY. I HAVE BEEN IN BED NOW FOR THE PAST 2 YEARS, GOING ON 3 AND I DON'T WANT TO DO THIS ANYMORE. I JUST WANT TO LIVE AGAIN...FIND SOME WAY OF GETTING BETTER. WHY NOT TRY THE TRADITIONAL CHINESE MEDICINE?..IT SURE ISN'T GOING TO HURT ME. AS A MATTER OF FACT, IT JUST MIGHT CURE ME.:)))<3 Karen
I RAN ACROSS THIS ARTICLE BELOW, TONIGHT AND FELT LIKE IT HAD HIT ON SOMETHING, THAT I HAVE BEEN JUST OVERLOOKING. I HAD TO GO TO THE DERMATOLOGIST BACK LAST YEAR FOR SOME SMALL BLISTERS THAT WERE COMING UP ON MY ARMS AND LEGS AND PLACES ON MY FACE. SHE TOLD ME THE REASON THAT THIS WAS HAPPENING, THAT MY HORMONES WERE OFF. SHE DID SAY THAT ONCE I HAD RETURNED TO MY USUAL HORMONE INJECTIONS OF REPLACEMENT THERAPY, THEN, I WILL BE JUST FINE AND I WAS BETTER FROM THAT STAND POINT AND GREATFUL FOR IT.:)
AS THE BREAKOUTS STARTED TO GRADUALLY COME BACK, I WONDERED IF IT WAS JUST HORMONAL. IT MADE ME THINK THERE COULD BE ANOTHER REASON 4 IT
.
I'VE WONDERED, IF THE HORMONAL THING COULD NOT BE THE EXACT REASON AND WHY, I WAS GETTING BLISTERS ON MY ARMS/LEGS AND SOME ON MY FACE. COULD IT BE ANOIHER REASON 4 IT?
THIS TIME, IT SEEMS TO BE DIFFERENT. I BURN LIKE FIRE ON THESE LITTLE PLACES THAT COME UP, MOSTLY ON MY ARMS. THEY DO LOOK AND FEEL LIKE SOMEONE HAS LITERALLY CUT ME OR SOMETHING AND WHEN THE TAKE A BAHT, THE WATER HITS IT AND IT REALLY BURNS.
I DO BELIEVE THAT MY BODY COULD BE DEALING WITH SOME KIND OF TOXICITY. MY MEDICATIONS MAYBE A REASON OR IT COULD JUST BE THE COMBINATION THAT THEY HAVE ME ON OR SOMETHING.
IT COULD BE AN AUTOIMMUNE DISEASE THAT JUST HASN'T BEEN RECOGNIZED OR FOUND AS OF YET AND THERE ARE SO MANY DIFFERENT KINDS OF AUTOIMMUNE DISEASES THAT A PERSONS HEAD COULD SPIN BECAUSE OF IT. I HAVEN'T BEEN DIAGNOSED WITH ONE ANY I AM SO GLAD I HAVEN'T. I AM TIRED OF WAITING FOR AN ANSWER. I AM DYING HERE, JUST A LITTLE BIT EVERYDAY.
I AM THINKING @ LOOKING UP THIS THING CALLED "SYDROME X" THAT I FOUND WHILE RESEARCHING THE NET. IT THAT IS ALL @ TOXICITY. WHO KNOWS, MAYBE, THIS ALL CAME FROM HAVING TO TAKE THIS STUPID MEDICINE THAT THEY HAVE ME ON, BUT I DONNO, I HAVE FELT THIS WAY FOR OVER 3 YRS AND THE MEDICINES THAT I HAVE TAKEN, HAVE BEEN THE SAME ONES FOR THE PAST 2 YRS. UNLESS, I HAVE DEVELOPED AN ALLERGY OR SOMETHING. IT IS POSSIBLE. SO, IF IT IS THAT I WILL BE SURPRISED THOUGH. IT COULD BE THE ANSWER.
WHEN I READ THIS, IT MADE SENSE. SO, I AM CALLING TO FIND ME A "TCM" DOC AS CLOSE AS I CAN. MAYBE, THEY CAN GET ME BACK UP ON MY FEET AGAIN. I AM PRAYING AND I HAVE FAITH. I AM NOT GOING TO GIVE UP, ALTHOUGH THERE HAS BEEN TIMES TO WHERE I FEEL I WON'T MAKE IT, BUT IT IS ALL UP TO THE LORD.:)))<3 Karen
HERE'S LINK TO THE SYNDROME "X" I WAS TALKING @
https://www.livehealthytoday.org/pages/syndrome-x.html
Acne - Traditional Chinese Medicine
I DON'T WANT TO LIVE HERE THE REST OF MY LIFE. I KNOW, IT IS HARD FOR ANYONE THAT DOESN'T EXPERIENCE THIS "NIGHTMARE", TO UNDERSTAND. IT IS UTTERLY IMPOSSIBLE FOR THAT TO HAPPEN, UNLESS U TRULY KNOW WHAT PAIN AND DISPAIR IS AND ARE OR HAVE FELT IT IN UR LIFE.
 I MUST SAY, I ONCE HAD A LIFE THAT WAS FULL AND BUSY. I LOVE TO WORK AND BE AROUND PEOPLE AND I LIKED THAT KIND OF LIFE. IT WAS A LIFE TO WHERE, WHEN U WAKE UP IN THE MORNING, U CAN PLAN UR DAY AND DO WHATEVER IT IS THAT NEEDED TO BE DONE.
I MUST SAY, I ONCE HAD A LIFE THAT WAS FULL AND BUSY. I LOVE TO WORK AND BE AROUND PEOPLE AND I LIKED THAT KIND OF LIFE. IT WAS A LIFE TO WHERE, WHEN U WAKE UP IN THE MORNING, U CAN PLAN UR DAY AND DO WHATEVER IT IS THAT NEEDED TO BE DONE. THAT IS DEFINITELY NOT MY LIFE NOW...NO, I LAY HERE AND SUFFER MOST OF THE TIME, BUT I DO THINK @ WHAT LIFE I HAVE HAD AND WAS BLESSED WITH. I COULD GO AND DO ANYTHING THAT I WANTED AND FELT SO ALIVE AND WELL, BUT NO NOW. NO, I DREAM A LOT AND THINK @ HOW MY LIFE USED TO BE AND I AM GREATFUL THAT I DID AT LEAST, GET TO EXPERIENCE WHAT I HAVE IN MY LIFE
I GOT TO SING AND GIVE MY MUSIC TO EVERYONE AND TO ME, IT WAS LIVING.:))
I AM GREATFUL GOD 4 THE LIFE YOU HAVE BLESSED ME WITH AND I THANK YOU 4 IT. I TRULY HAVE HAD A WONDERFUL LIFE, BUT IT SURE CHANGED ON ME SO FAST.
PLEASE LORD, GIVE ME SOME OF MY LIFE BACK. HELP ME TO BE THE MOM THAT I NEED TO BE. I KNOW THEY HAVE DONE WITHOUT ME, MANY TIMES AND WANTED ME TO BE THERE, BUT I COULDN'T. I WASN'T ABLE...GOD KNOWS, IT IS TRUE.
IF THERE WAS ANYTHING I COULD'VE DONE TO BE THERE, I WOULD DO, BUT UNFORTUNATELY...MOM WASN'T ABLE AND THAT IS THE GODS HONEST TRUTH.
IF I HAD A CHOICE IN THE MATTER I WOULD ALWAYS MAKE EACH AND EVERY FUNCTION OR IMPORTANT TIME THAT U WANTED ME TO BE THERE. IT HAS HURT ME SO MUCH...MORE THAN U KNOW TO NOT HAVE BEEN ABLE OR CAPABLE TO BE THERE AND I AM SORRY TO THE BOTTOM OF MY HEART. IT HAS TO BE ONE OF THE HARDEST THINGS FOR A MOM TO HAVE TO DO...BE AWAY FROM MY SONS.
 I KNOW, THEY HAVE MISSED ME, ON MORE THAN ONE OCASION AND I AM TRULY SORRY. MOM IS TELLING THE TRUTH. AS BAD AS I HATE TO SAY IT...I AM REALLY SICK AND IT SEEMS THAT NO ONE IS TAKING ME SERIOUSLY. WHY IS IT SO HARD FOR PEOPLE TO SEE JUST SICK I AM? I CAN'T STAND ON MY OWN TWO FEET FOR 5 MINUTES, B4 I START FEELING MY BACK START TO BURN. IT STARTS IN MY RIBS AND IT WILL COVER MY BACK. I AM TALKING @ A SHEET OF FIRE AND I HAVE TO FIND SOMEWHERE TO LEAN BACK STRAIGHT ON (that is the only thing that will give me a minute b4 I have to get to the bed and fast)OR IT WILL GET SO BAD THAT THE PAIN IS SO EXCRUCIATING AND IT IS HORRIBLE.:((
I KNOW, THEY HAVE MISSED ME, ON MORE THAN ONE OCASION AND I AM TRULY SORRY. MOM IS TELLING THE TRUTH. AS BAD AS I HATE TO SAY IT...I AM REALLY SICK AND IT SEEMS THAT NO ONE IS TAKING ME SERIOUSLY. WHY IS IT SO HARD FOR PEOPLE TO SEE JUST SICK I AM? I CAN'T STAND ON MY OWN TWO FEET FOR 5 MINUTES, B4 I START FEELING MY BACK START TO BURN. IT STARTS IN MY RIBS AND IT WILL COVER MY BACK. I AM TALKING @ A SHEET OF FIRE AND I HAVE TO FIND SOMEWHERE TO LEAN BACK STRAIGHT ON (that is the only thing that will give me a minute b4 I have to get to the bed and fast)OR IT WILL GET SO BAD THAT THE PAIN IS SO EXCRUCIATING AND IT IS HORRIBLE.:(( I MUST SAY THIS IS ONE OF CREEPIEST, SCARRIEST FEELINGS A PERSON CAN ECER HAVE. IT FEELS LIKE UR HAVING A STROKE. NOW, ONE TIME,WHILE ALL THIS WAS HAPPENING...THE WHOLE LEFT SIDE OF MY BODY WENT COMPLETELY LIMP. I COULDN'T MOVE, AT ALL. I HAD TO CALL 911, BECAUSE I COULDN'T MOVE THE WHOLE LEFT SIDE OF MY BODY, AT ALL. IT WAS PARALYSED COMPLETELY. I FELT LIKE A 40LB. WEIGHT WAS LAYING ON MY LEFT ARM AND LEG. I THOUGHT FOR SURE THAT I WAS HAVING A STROKE. WHAT ELSE COULD IT BE?..A HEART ATTACK, MAYBE, I DONNO I AM THE ONE WHOS BRAIN IS NUMB..LITERALLY AND SCARED OUT OF MY MIND THINKING...WELL, THIS IS IT.
WOULDN'T U WANT TO KNOW WHAT CAUSED UR BODY TO GO COMPLETELY NUMB AND TO DO THIS?...WHY OF COURSE U WOULD. GUYS, I AM JUST TIRED AND KNOW THERE IS SOMEONE WRONG AND IT HAS GOT TO BE FOUND. THERE IS SOMEONE OUT THERE THAT HELP ME..SURELY THERE IS SOMEONE THAT CAN FIX ME.
I THINK, I MADE THE MISTAKE OF THINKING A NEUROLOGIST WAS THE ANSWER TO WHAT I HAVE, I GUESS. NOW, I AM LEANING TOWARD SEEING AN ENDOCRINOLOGIST, AN ONCOLOGIST AND AN INFECTIOUS DISEASE DOC. I ONLY THINK THAT SINCE I HAVE A LOT OF PROBLEMS WITH MY BLOOD THAT IS WHERE I SHOULD START, BUT IN THE MEANTIME, IT WON'T HURT ME TO CHECK OUT THE TCM. IT MIGHT HELP ME, SO IT IS WORHT A TRY.:)
THIS TRADITIONAL CHINESE MEDICINE. IT IS ALL NATURAL AND MAYBE WHAT MY BODY NEEDS. IT IS WORTH A TRY. I HAVE HEARD SO MANY EXCELLENT OUTCOMES FROM IT. I AM JUST READY TO GET THIS SITUATION TO CHANGE. IT HAS TO, SOMEWAY.
I KNOW THAT THIS HAS GONE ON FOR TOO LONG (it started in '03, with just a neck pain and i couldn't sleep and wound up with surgery that took my C5-C6 out) I JUST KNOW THAT THIS IS RIDICULAS THAT THE DOCS CAN'T GIVE ME AN ANSWER.
AGAIN, I HAVE ONLY BEEN GOING TO SEE NEUROLOGISTS, ALL THIS TIME AND THINK THAT THIS WAS MY FIRST MISTAKE. I SHOULD'VE GONE TO SEE SOME OTHER KINDS OF DOCTORS...I SEE THAT NOW, BUT, I WAS HURTING IN MY NECK AND FELT IT WAS SOME KIND OF MECHANICAL PROBLEM THAT HAS GONE WRONG WITH THE TITANIUM PLATES OR THE SCREWS THAT HELD THEM IN PLACE.

THE PICTURE ABOVE, SHOWS THE SWELLING IN MY FACE(moon face) AND MY OVERALL BODY WEIGHT GOT UP TO 199...WOW, I WAS FAT AND MISERABLE. NOW, AT LEAST, I AM BACK DOWN TO 145 AND THAT IS SOMETHING, BUT THE PAIN IS STILL THERE.
I DON'T KNOW WHAT HAS ME, I JUST KNOW THAT I AM LIVING BASICALLY A "HELL ON EARTH" SCENERIO ,RIGHT NOW. (forgive me Lord..don't mean that disrespectfully in any way) BECAUSE, ANYWAY THAT U LOOK AT IT, I AM STILL BLESSED.:))<3
I DO KNOW GOD HAS A REASON 4 EVERYTHING AND AS LONG AS HE IS IN CONTROL, I WILL ACCEPT WHAT MY LIFE IS BECAUSE I KNOW GOD IS IN CONTROL. I WILL ALSO CONTINUE TO FIGHT TO FIND THE ANSWERS AND TRY TO GET MY LIFE BACK... AND WHO WOULDN'T?
WE ARE SUPPOSE TO STRIVE TO LIVE A GOOD LIFE AND TO LIVE IT FOR THE LORD. HE GAVE US EVERYTHING...HE EVEN GAVE US HIS LIFE AND I KNOW THAT I AM GREATFUL. I WAS BLESSED WITH TWO WONDERFUL PARENTS, THAT LOVE AND TAKE GOOD CARE OF ME. MOM COOKS ALL THE TIME AND SHE IS NOT WELL. I WORRY @ HER AND WHAT SHE TRIES TO DO FOR ME. SHE PUSHES HERSELF SO HARD, BUT I CAN SEE IT. I CAN SEE THAT SHE ISN'T WELL. AFTER ALL, SHE DOES HAVE A CYST ON HER LIVER. AND DAD RUNS ALL THE TIME DRIVING ME HERE AND THERE...IF, I CAN GO THAT IS AND HAVE A DAY TO WHRE, I CAN AT LEAST, GET READY TO GO.

 I NEED TO GET WELL, SO I CAN TAKE CARE OF THEM FOR A CHANGE. I PRAY THAT IS SOON, LORD. I WANT AND NEED TO BE ABLE TO SPEND MORE TIME LAUGHING, FISHING, EATING, SINGING AND LOVING AND LIVING MY LIFE...BUT, THIS TIME LORD...U WILL BE RIGHT THERE BESIDE ME, ALL THE WAY.:)))<3
I NEED TO GET WELL, SO I CAN TAKE CARE OF THEM FOR A CHANGE. I PRAY THAT IS SOON, LORD. I WANT AND NEED TO BE ABLE TO SPEND MORE TIME LAUGHING, FISHING, EATING, SINGING AND LOVING AND LIVING MY LIFE...BUT, THIS TIME LORD...U WILL BE RIGHT THERE BESIDE ME, ALL THE WAY.:)))<3 REGARDLESS OF MY PAIN, I DO HAVE A GOOD LIFE, BUT MAYBE THIS IS A LESSON THAT I NEEDED TO LEARN. I DO KNOW THAT I REALLY HAVE BEEN HUMBLED, SINCE I GOT SICK. IT HAS CHANGED MY LIFE...ONLY 4 THE BETTER, BECAUSE I KNOW GOD AND THAT IS MORE IMPORTANT THAN ANYTHING, IN THE WORLD. I AM SO GLAD, I AM HIS.:D
I AM GLAD THAT I FOUND HIM...AND THAT HE FOUND ME.:)))
DEAR LORD, U KNOW WHAT I AM GOING THROUGH AND I PRAY THAT MY LIFE IS GOING TO CHANGE, IF IT IS UR WILL...TO WHERE I CAN JUST WALK AROUND AND BE HAPPY AGAIN. I PRAY 4 MY FAMILY TO GET THROUGH THIS AND TO UNDERSTAND IT ALL. I REALLY BELIEVE THAT SOMETHING IS SEIOUSLY WRONG WITH ME AND I HOPE THAT IT DOESN'T TAKE ME AWAY FROM HERE JUST YET. IF IT IS "UR WILL LORD". I JUST WOULD LOVE TO ENJOY MY FAMILY AND DO THINGS WITH THEM AGAIN. I JUST MISSED OUT ON SO MUCH AND SO MANY THINGS WITH MY FAMILY I WANT TO MAKE THAT UP, IF I CAN. I REALLY NEED AN ADVOCATE, LORD..TO FIGHT TO GET ME WELL.
DEAR LORD, SEND ME AN ADVOCATE BECAUSE MY MOM AND DAD DON'T KNOW WHAT TO DO TO FIND OUT WHAT IS WRONG WITH MEAND I KNOW THEY ARE SO TIRED. MY HUSBAND, WORKS ALL THE TIME AND THAT MAKES IT HARD TO DEDICATE ANY TIME, TO TRAVEL AND GO TO DOCS.
LORD, EVERYDAY I BATTLE THIS PAIN AND I PRAY THAT I WILL GET WELL. I DO ALSO PRAY THAT NO ONE HAS TO FEEL THIS PAIN, IF I MAY BECAUSE IT IS SO BAD. ...AND I JUST WANT IT TO BE OVER. I KNOW, LORD...YOU HAVE KEPT ME HERE AND I AM THANKFUL 4 THAT. :D
PLEASE ANSWER MY PRAYER LORD AND GET ME WELL.:)<3

WELL, I MUST SAY THAT I HAVE REALLY TRIED TO SEE IF THE WESTERN MEDICINE COULD HELP ME, BUT I AM NOT GETTING ANY BETTER. I AM STILL IN PAIN AND AS A MATTER OF FACT, I AM GETTING WORSE(sad 2 say). SO, I HAVE TO DO SOMETHING TO GET WELL BECAUSE THIS PAIN IS EVERYDAY, ACTUALLY FEELS LIKE IT COULD KILL ME SOMETIMES, BUT I KEEP MOVING ON...AND IT DOES GET VERY VERY OLD TO DEAL WITH.
ALSO, I DO KNOW THAT IT MUST BE HARD ON THE ONES I LOVE AND THAT LOVES ME. I CAN ONLY IMAGINE IT BEING ONE OF MY KIDS. MY HEART WOULD BE BROKEN. I WOULDN'T WANT TO SEE THEM LIKE THAT. SO, I KNOW MY MOM AND DAD HAVE REALLY WORRIED @ ME AND HAVE BEEN THROUGH IT. SO MANY TIMES HAVE THEY GOT UP EARLY IN THE MORNING TO DRIVE ME TO ANOTHER DOC OR HAD TO SIT AND WATCH ME SCREAM OUT IN PAIN. IT MAKES ME SAD THAT THEY ARE HAVING TO GO THROUGH THAT, BUT I DON'T KNOW WHAT TO DO THAT COULD MAKE IT ANY EASIER ON THEM??;(
I AM THE ONE SUFFERING HERE AND IT IS HARD, WHEN SOMETHING SO PAINFUL HAS A HOLD OF U AND IT DOESN'T JUST STOP OR LET UP...NO, IT EASES UP SOME AND I CAN BREATH WITH SOME ~SIGH~ OF RELIEF...UNTIL, IT COMES BACK.
IT IS HORRIBLE AND SO DEBILITATING AND EXCRUCIATING AT TIMES, I FEEL LIKE I AM HAVING A STROKE OR SOMETHING,FOR THE WHOLE LEFT SIDE OF MY BODY GOES COMPLETELY NUMB AND IT HAS GONE COMPLETELY PARALYZED ON MY LEFT SIDE. THAT IS BAD.
THIS CAN BE A SIGN OF "MS", BUT I HAVEN'T BEEN DIAGNOSED WITH THAT AND AM GLAD, BUT AND YES, THERE IS A BUT IN THERE. THE DOCS DID FIND A LESION ON MY THORACIC AND THE THE NEUROLOGIST THAT FOUND IT SAID THAT IT WAS OUT OF HIS AREA OF EXPERTISE AND JUST LEFT ME HANGING WITH NO ONE TO GO TO OR SEE. I JUST WANT TO SEE SOMEONE THAT HAS EXPERTISE, BUT WHERE ARE THEY? IT IS HARD TO FIND A DECENT DOC THAT WON'T TREAT U LIKE A SWINGING DOOR..."NEXT". I HOPE THAT I DON'T HAVE MS AND THEY HAVEN'T SAID I HAVE THAT YET AND I AM PRAYING THAT I DON'T.
I DO KNOW THAT SOMETHING IS TERRIBLY WRONG, BUT I AM NOT A DOCTOR. ALL I CAN DO IS RESEARCH AND BE INFORMED OF THE POSSIBILITIES. I NEVER TRY TO DIAGNOSE MYSELF, I ONLY COMPARE ALL OF THE SYMPTOMS OF SOMETHING AND THEN, I WRITE THAT DOWN AND COMPARE FROM THE LIST. I THEN, TAKE MY THEORIES TO THE DOC TO SEE, IF THEY SAY IT IS A POSSIBILITY OR NOT. THERE IS SO MANY DIFFERENT POSSIBILITIES OF WHAT IT COULD BE. WE HAVE TO BASICALLY BE OUR OWN BE ADVOCATES SOMETIMES, BUT I AM TIRED AND NEED HELP.
NO, I CAN'T DIAGNOSE MYSELF, NO ONE CAN AND IT MUST SEEM THAT WAY BECAUSE, I POST SO MANY DIFFERENT ARTICLES AND @ MANY DIFFERENT THINGS. THE ONLY REASON I DO IS BECAUSE I FIND IT INTERESTINGLY ENOUGH, TO SAVE IT AS A SORT OF DOCUMENTATION OF WHAT I AM GOING THROUGH AND ALSO, TO SHARE IT WITH OTHERS. I KNOW, THERE COULD BE OTHERS THAT COULD HAVE A PARTICULAR INTEREST, IN SAID SUCH ARTICLE, SO I POST IT FOR ALL.
I DO THINK OF OTHERS AND TO ME...MY MOTTO WOULD BE, "I WOULD RATHER BE INFORMED, THAN UNINFORMED"...ESPECIALLY, WHEN IT COMES TO OUR HEALTH. THESE DAYS, IT IS WAY TOO IMPORTANT TO TRY TO STAY AS HEALTHY AS WE CAN.
I HAVE BEEN GOING TO DOCS AND TELLING THEM WHAT I FEEL AND WHAT I GO THROUGH AND THEY HAVE MADE DIANOSIS'S AND PRESCRIBED THERAPY, MEDICINES AND RUN MANY TESTS, BUT THEY HAVEN'T FOUND THE ELUSIVE ONE YET...NO, NOT THE ONE THAT IS KEEPING ME IN THIS BED!
I AM SO TIRED OF SEEING DOCTORS THAT ARE NOT FINDING THE ANSWER TO WHAT IT IS THAT IS MAKING ME SICK AND IN SO MUCH PAIN. SO, THAT IS WHY I AM LOOKING FOR SOMEONE THAT PRACTICES TCM. I FEEL IF IT CAN CURE SOME CANCERS, IT POSSIBLY COULD CURE ME.
ONE MORE WORD OR TWO B4 I GO. I DO KNOW THAT IT IS HARD TO UNDERSTAND WHAT SOMEONE IS GOING THROUGH AND NOT MANY PEOPLE CAN RELATE TO SOMEONE ELSE'S PAIN, NOT TOTALLY. I AM IN CHRONIC PAIN AND I AM SO TIRED.
I MUST FIND AN ANSWER TO WHAT IS TAKING MY LIFE AND THROWING IT ALL AWAY. I HAVE BEEN IN BED NOW FOR THE PAST 2 YEARS, GOING ON 3 AND I DON'T WANT TO DO THIS ANYMORE. I JUST WANT TO LIVE AGAIN...FIND SOME WAY OF GETTING BETTER. WHY NOT TRY THE TRADITIONAL CHINESE MEDICINE?..IT SURE ISN'T GOING TO HURT ME. AS A MATTER OF FACT, IT JUST MIGHT CURE ME.:)))<3 Karen
I RAN ACROSS THIS ARTICLE BELOW, TONIGHT AND FELT LIKE IT HAD HIT ON SOMETHING, THAT I HAVE BEEN JUST OVERLOOKING. I HAD TO GO TO THE DERMATOLOGIST BACK LAST YEAR FOR SOME SMALL BLISTERS THAT WERE COMING UP ON MY ARMS AND LEGS AND PLACES ON MY FACE. SHE TOLD ME THE REASON THAT THIS WAS HAPPENING, THAT MY HORMONES WERE OFF. SHE DID SAY THAT ONCE I HAD RETURNED TO MY USUAL HORMONE INJECTIONS OF REPLACEMENT THERAPY, THEN, I WILL BE JUST FINE AND I WAS BETTER FROM THAT STAND POINT AND GREATFUL FOR IT.:)
AS THE BREAKOUTS STARTED TO GRADUALLY COME BACK, I WONDERED IF IT WAS JUST HORMONAL. IT MADE ME THINK THERE COULD BE ANOTHER REASON 4 IT
.
I'VE WONDERED, IF THE HORMONAL THING COULD NOT BE THE EXACT REASON AND WHY, I WAS GETTING BLISTERS ON MY ARMS/LEGS AND SOME ON MY FACE. COULD IT BE ANOIHER REASON 4 IT?
THIS TIME, IT SEEMS TO BE DIFFERENT. I BURN LIKE FIRE ON THESE LITTLE PLACES THAT COME UP, MOSTLY ON MY ARMS. THEY DO LOOK AND FEEL LIKE SOMEONE HAS LITERALLY CUT ME OR SOMETHING AND WHEN THE TAKE A BAHT, THE WATER HITS IT AND IT REALLY BURNS.
I DO BELIEVE THAT MY BODY COULD BE DEALING WITH SOME KIND OF TOXICITY. MY MEDICATIONS MAYBE A REASON OR IT COULD JUST BE THE COMBINATION THAT THEY HAVE ME ON OR SOMETHING.
IT COULD BE AN AUTOIMMUNE DISEASE THAT JUST HASN'T BEEN RECOGNIZED OR FOUND AS OF YET AND THERE ARE SO MANY DIFFERENT KINDS OF AUTOIMMUNE DISEASES THAT A PERSONS HEAD COULD SPIN BECAUSE OF IT. I HAVEN'T BEEN DIAGNOSED WITH ONE ANY I AM SO GLAD I HAVEN'T. I AM TIRED OF WAITING FOR AN ANSWER. I AM DYING HERE, JUST A LITTLE BIT EVERYDAY.
I AM THINKING @ LOOKING UP THIS THING CALLED "SYDROME X" THAT I FOUND WHILE RESEARCHING THE NET. IT THAT IS ALL @ TOXICITY. WHO KNOWS, MAYBE, THIS ALL CAME FROM HAVING TO TAKE THIS STUPID MEDICINE THAT THEY HAVE ME ON, BUT I DONNO, I HAVE FELT THIS WAY FOR OVER 3 YRS AND THE MEDICINES THAT I HAVE TAKEN, HAVE BEEN THE SAME ONES FOR THE PAST 2 YRS. UNLESS, I HAVE DEVELOPED AN ALLERGY OR SOMETHING. IT IS POSSIBLE. SO, IF IT IS THAT I WILL BE SURPRISED THOUGH. IT COULD BE THE ANSWER.
WHEN I READ THIS, IT MADE SENSE. SO, I AM CALLING TO FIND ME A "TCM" DOC AS CLOSE AS I CAN. MAYBE, THEY CAN GET ME BACK UP ON MY FEET AGAIN. I AM PRAYING AND I HAVE FAITH. I AM NOT GOING TO GIVE UP, ALTHOUGH THERE HAS BEEN TIMES TO WHERE I FEEL I WON'T MAKE IT, BUT IT IS ALL UP TO THE LORD.:)))<3 Karen
HERE'S LINK TO THE SYNDROME "X" I WAS TALKING @
https://www.livehealthytoday.org/pages/syndrome-x.html
Acne - Traditional Chinese Medicine
In Traditional Chinese Medicine (TCM), acne is considered a disease primarily related to the Pathogenic Influence of Heat and Damp Heat on the meridians, Zang Fu, and Fundamental Substances. This Heat may be a product of poor diet, stress, overwork, a congenital condition, or the natural ascendance of Yang energy, which is typical in adolescence.
Heat may affect the Lung or Stomach Meridians, from where it is transmitted to the skin of the face and chest, causing the condition's inflammatory response. If the Heat tries to escape from the Tai Yang channel, acne occurs on the back. Heat usually is exacerbated in the Lung Meridian by the External Wind Pathogen, which causes skin redness. In the Stomach Meridian, it can be aggravated by a diet of greasy and spicy foods, which weakens and creates more Damp Heat in the Spleen Zang and the Stomach Fu.
Heat also may enter into the Blood or transmute into Toxic Heat, both of which can cause lesions. Finally, emotional health can contribute to acne. Extreme emotions of sadness, anxiety, stress, or anger can cause Disharmony in the body. This can lead to stagnation of Qi and cause Heat and Dampness to rise to the skin.
Traditional Chinese Medicine Categories of Acne
In TCM, Heat affects the different Meridians, Zang Fu Organs, and Fundamental Substances, providing the substratum that allows acne to occur. The different manifestations of Heat in these aspects of the body's energetics appear as different complexes of signs and symptoms. Acne requires a careful differentiation of Heat so that proper treatment can be formulated to match the Pattern of Disharmony.
Lung Heat and Stomach Heat are the most common forms of acne. If Dampness is present, the skin will be greasy. Sores and bleeding signify toxicity. Itchiness can be caused by Wind and Dampness. The most common form of itchiness in acne is from Wind that arises from Heat.
Lung Heat: Symptoms include acne with a predominance of lesions on the forehead and near the nose. There may be slight itching as well. In cases with a rapid onset of new lesions, the patient may complain of chills or sensitivity to Wind. The patient may have an aversion to heat and feel thirsty. The tongue is generally red with a thin yellow coat, and the pulse may be rapid and floating.
Stomach Heat: Symptoms include acne with a predominance of lesions around the mouth and on the chest, shoulders, and back. The patient may have an aversion to heat; have a large appetite and thirst; and prefer greasy, spicy foods. There may be a tendency to pass dry stools as well. The tongue is usually red with a thick yellow coating, and the pulse is rapid and forceful.
Toxic Heat: Symptoms include severe acne, strongly inflamed with pus-filled nodules and much reddening of the skin around the lesions. The patient may have an aversion to heat as well and may complain of malaise. The tongue is generally red with a dry yellow coating, and the pulse is rapid.
Damp Heat: Symptoms include acne composed of deep, pus-filled, inflamed nodules. The skin usually is oily, and the patient may have an aversion to heat. He or she may be thirsty but have no desire to take fluids. The tongue generally is red or crimson, with a greasy or sticky coating. The pulse is rapid and may have slippery or wiry qualities as well.
Blood Heat: Symptoms include acne that is accompanied by a flushed face and strong aversion to heat. The patient may complain of thirst, dark urine, and dry stools. The tongue usually is red (with a redder tip) and has a yellow coating, or may be crimson in color. The pulse usually is rapid and thin.
Heat may affect the Lung or Stomach Meridians, from where it is transmitted to the skin of the face and chest, causing the condition's inflammatory response. If the Heat tries to escape from the Tai Yang channel, acne occurs on the back. Heat usually is exacerbated in the Lung Meridian by the External Wind Pathogen, which causes skin redness. In the Stomach Meridian, it can be aggravated by a diet of greasy and spicy foods, which weakens and creates more Damp Heat in the Spleen Zang and the Stomach Fu.
Heat also may enter into the Blood or transmute into Toxic Heat, both of which can cause lesions. Finally, emotional health can contribute to acne. Extreme emotions of sadness, anxiety, stress, or anger can cause Disharmony in the body. This can lead to stagnation of Qi and cause Heat and Dampness to rise to the skin.
Traditional Chinese Medicine Categories of Acne
In TCM, Heat affects the different Meridians, Zang Fu Organs, and Fundamental Substances, providing the substratum that allows acne to occur. The different manifestations of Heat in these aspects of the body's energetics appear as different complexes of signs and symptoms. Acne requires a careful differentiation of Heat so that proper treatment can be formulated to match the Pattern of Disharmony.
Lung Heat and Stomach Heat are the most common forms of acne. If Dampness is present, the skin will be greasy. Sores and bleeding signify toxicity. Itchiness can be caused by Wind and Dampness. The most common form of itchiness in acne is from Wind that arises from Heat.
Friday, November 4, 2011
WE NEED TO BE TAKEN SERIOUSLY B4 IT TURNS OUT TOO LATE TO CHANGE ANYTHING
THIS IS ANOTHER EXAMPLE OF A PERSON HAVING ISSUES WITH PAIN AND WAS MADE TO WAIT TOO LONG B4 THEY FOUND WHAT WAS CAUSING THE PAIN. NOW, HE HAS TO LIVE WITH THE DEBILITATING PAIN EACH AND EVERY DAY. THIS PERSON, ALSO HAD A CERVICAL SURGERY (like I did) AND HE WOUND UP WITH COMPLICATIONS FOLLOWING.
IT MAKES A PERSON WONDER JUST WHY THEY WON'T LOOK BEHIND MY TITANIUM PLATES. THAT IS ALL I WANT DONE. IF YOU CAN'T SEE BEHIND TITANIUM PLATES FROM A PREVIOUS NECK SURGERY AND HAVE BEEN SUFFERING FOR 6 YRS. OR MORE AND CAN'T RECEIVE AN ANSWER TO WHY THE SUFFERING HAS TO CONTINUE. WHEN, IT IS VERY POSSIBLE TO REMOVE THE PLATES SO THAT THE NEUROSURGEN CAN GET A COMPLETE VIEW OF THE AREA AND MAKE SURE THAT THE PROBLEM ISN'T COMING FROM THIS AREA, IN THE FIRST PLACE. I HAVE TO RULE OUT ANY CONNECTION TO THE POSSIBLE CAUSE OF THIS DEBILITATING AND EXCRUCIATING PAIN THAT THE I EXPERIENCE EVERYDAY.
 A PATIENT SHOULDN'T HAVE TO GO THROUGH ANY AMOUNT OF PAIN...ON A DAILY BASIS, IF THEY CAN FIND THE CULPRIT. I REALLY THINK, THE PLATES SHOULD BE REMOVED AND THE AREA FULLY VIEWED, BECAUSE THERE HAS YET TO BE A SOLUTION TO THIS PROBLEM. WHY DOES IT HURT TO JUST LOOK? MAYBE, THEY CAN PUT SOME KIND OF CAMERA IN AND TAKE A PEEK OR SOMETHING. ANYTHING, BUT NOTHING!!! I DON'T UNDERSTAND WHY THEY WOULD JUST SUBJECT ME TO LIVE IN THIS MISERY THE REST OF MY LIFE...THE WAY I AM LIVING, WHEN TO ME, THIS IS NOT LIVING. ONE MORE THING, I AM NOT STRETCHING THIS. THIS PAIN IS REAL AND HORRYFYING, AT TIMES.
A PATIENT SHOULDN'T HAVE TO GO THROUGH ANY AMOUNT OF PAIN...ON A DAILY BASIS, IF THEY CAN FIND THE CULPRIT. I REALLY THINK, THE PLATES SHOULD BE REMOVED AND THE AREA FULLY VIEWED, BECAUSE THERE HAS YET TO BE A SOLUTION TO THIS PROBLEM. WHY DOES IT HURT TO JUST LOOK? MAYBE, THEY CAN PUT SOME KIND OF CAMERA IN AND TAKE A PEEK OR SOMETHING. ANYTHING, BUT NOTHING!!! I DON'T UNDERSTAND WHY THEY WOULD JUST SUBJECT ME TO LIVE IN THIS MISERY THE REST OF MY LIFE...THE WAY I AM LIVING, WHEN TO ME, THIS IS NOT LIVING. ONE MORE THING, I AM NOT STRETCHING THIS. THIS PAIN IS REAL AND HORRYFYING, AT TIMES.
I FEEL THAT I HAVE BEEN BASICALLY BEGGING TO GET THESE PLATES REMOVED, SO THAT A FULL COMPREHENSIVE VIEW OF THE POSSIBLE AREA THAT IS APPARANTLY HAVING MORE PROBLEMS THAT I CAN STAND...CAN BE VIEWED AND THEN THEY CAN RULE IT OUT, IF THERE IS NO PROBLEM BEHIND THEM, BUT DON'T ASSUME THAT THERE IS NOTHING IN THERE. I FEEL IT AND I KNOW THAT SOMETHING IS WRONG SOMEWHERE. IS THAT ASKING TOO MUCH?...NO. THEY CAN'T SEE BEHIND THEM AND I AM DYING HERE. I MUST SAY, THAT IS WHAT IT FEELS LIKE ANYWAY. AT LEAST, I WISH THEY WOULD LOOK, SO I CAN MOVE ON TO FIND THE ANSWER, INSTEAD OF JUST LAYING HERE WITHERING AWAY. NO, I MUST AND CAN FIND THE ANSWER...SOMEHOW.

MY BODY IS TIRED OF BEING IN PAIN. WHY CAN'T SOMEONE SEE THAT? WHY CAN'T SOMEONE MAKE THEM LOOK FURTHER...DEEPER TO FIND THE PROBLEM, INSTEAD OF COVERING IT UP OR TRYING TO MASK MY SYMPTOMS BY MEDICATING ME. WELL, MY SYMPTOMS ARE BECOMING A VERY BIG PROBLEM. THEY ARE TAKING MY LIFE AWAY FROM ME AND I AM TIRED NOW AND I HAVE TO FIGHT BACK OR I WILL BE IN MY GRAVE, AT AN EARLY AGE. I KNOW THAT DOES SOUND MORBID, BUT IT IS TRUE. IF A PERSON DOESN'T FIGHT TO LIVE...THEY WON'T MAKE IT.
THIS HAS NEEDED TO BE ATTENDED TO FOR A LONG TIME NOW. NOW, I AM IRATE AND ANGRY BECAUSE I HAVE BEEN LEFT HERE TO FEND FOR MYSELF...BASICALLY. I AM ONE OF THE LUCKY ONES THAT DOES HAVE SOMEONE TO AT LEAST TEND TO ME AND HELP ME GET THROUGH MY DAYS AND I AM SO GREATFUL THAT I DO, BUT WHAT @ THE PEOPLE WHO DON'T HAVE ANYONE TO HELP THEM? THEY ARE OUT THERE.:(
I WANT TO LIVE AGAIN AND ALL I HAVE IS THIS COMPUTER TO SAY WHAT IT IS THAT I NEED TO SAY, BECAUSE IT IS VERY EVIDENT THAT GOING TO DOCTORS ASKING THEM TO HELP FIND WHAT IT IS THAT IS KILLING ME...GETTING VERY OLD AND I AM GETTING NO WHERE, IN THE PROCESS.
AFTER DEALING WITH A CERVICAL SURGERY, I SHOULD AT LEAST HAVE THE RIGHT TO KNOW, IF THERE IS SOMETHING WRONG IN THERE AND NOT BE JUST LEFT IN THE DARK @ IT.
THIS PERSON BELOW, NAMED "JS", IS SUFFERING AND HE, LIKE ME, HAD A CERVICAL DISKECTOMY, BUT IT WAS TOO LATE FOR HIM TO EVER REGAIN HIS LIFE BACK, LIKE IT ONCE WAS..AGAIN.
IT JUST TOOK TOO LONG TO GET ANYONE TO LISTEN TO HIM AND I KNOW HOW HE FEELS. THIS IS ONE OF THE THINGS THAT I AM AFRAID OF, IT TAKING TOO LONG TO FIND THE CULPRIT.
THIS IS JUST AN EXAMPLE OF WHAT CAN HAPPEN AND THIS COULD HAVE BEEN AVOIDED, IF ONLY A DOCTOR WOULD HAVE SEEN THE SIGNS ,B4 IT WAS TOO LATE. HE DIDN'T GET HIS ANSWER FAST ENOUGH AND BY NOT FINDING WHAT IT WAS THAT WAS SO IMPORTANT, HE WOUND UP HAVING PRESSURE ON HIS SPINAL CORD,4 TOO LONG.
IT, ALL CAME DOWN TO THE DOCTOR, NOT TRYING HARD ENOUGH TO GET TO THE BOTTOM OF IT. THIS PROBABLY COULD HAVE BEEN AVOIDED, IF ONLY THE PATIENT, WOULD HAVE BEEN LISTENED TO, IN THE FIRST PLACE .
YEAH, WE DO KNOW OUR BODIES.
JS in SD
IT MAKES A PERSON WONDER JUST WHY THEY WON'T LOOK BEHIND MY TITANIUM PLATES. THAT IS ALL I WANT DONE. IF YOU CAN'T SEE BEHIND TITANIUM PLATES FROM A PREVIOUS NECK SURGERY AND HAVE BEEN SUFFERING FOR 6 YRS. OR MORE AND CAN'T RECEIVE AN ANSWER TO WHY THE SUFFERING HAS TO CONTINUE. WHEN, IT IS VERY POSSIBLE TO REMOVE THE PLATES SO THAT THE NEUROSURGEN CAN GET A COMPLETE VIEW OF THE AREA AND MAKE SURE THAT THE PROBLEM ISN'T COMING FROM THIS AREA, IN THE FIRST PLACE. I HAVE TO RULE OUT ANY CONNECTION TO THE POSSIBLE CAUSE OF THIS DEBILITATING AND EXCRUCIATING PAIN THAT THE I EXPERIENCE EVERYDAY.
I FEEL THAT I HAVE BEEN BASICALLY BEGGING TO GET THESE PLATES REMOVED, SO THAT A FULL COMPREHENSIVE VIEW OF THE POSSIBLE AREA THAT IS APPARANTLY HAVING MORE PROBLEMS THAT I CAN STAND...CAN BE VIEWED AND THEN THEY CAN RULE IT OUT, IF THERE IS NO PROBLEM BEHIND THEM, BUT DON'T ASSUME THAT THERE IS NOTHING IN THERE. I FEEL IT AND I KNOW THAT SOMETHING IS WRONG SOMEWHERE. IS THAT ASKING TOO MUCH?...NO. THEY CAN'T SEE BEHIND THEM AND I AM DYING HERE. I MUST SAY, THAT IS WHAT IT FEELS LIKE ANYWAY. AT LEAST, I WISH THEY WOULD LOOK, SO I CAN MOVE ON TO FIND THE ANSWER, INSTEAD OF JUST LAYING HERE WITHERING AWAY. NO, I MUST AND CAN FIND THE ANSWER...SOMEHOW.
MY BODY IS TIRED OF BEING IN PAIN. WHY CAN'T SOMEONE SEE THAT? WHY CAN'T SOMEONE MAKE THEM LOOK FURTHER...DEEPER TO FIND THE PROBLEM, INSTEAD OF COVERING IT UP OR TRYING TO MASK MY SYMPTOMS BY MEDICATING ME. WELL, MY SYMPTOMS ARE BECOMING A VERY BIG PROBLEM. THEY ARE TAKING MY LIFE AWAY FROM ME AND I AM TIRED NOW AND I HAVE TO FIGHT BACK OR I WILL BE IN MY GRAVE, AT AN EARLY AGE. I KNOW THAT DOES SOUND MORBID, BUT IT IS TRUE. IF A PERSON DOESN'T FIGHT TO LIVE...THEY WON'T MAKE IT.
THIS HAS NEEDED TO BE ATTENDED TO FOR A LONG TIME NOW. NOW, I AM IRATE AND ANGRY BECAUSE I HAVE BEEN LEFT HERE TO FEND FOR MYSELF...BASICALLY. I AM ONE OF THE LUCKY ONES THAT DOES HAVE SOMEONE TO AT LEAST TEND TO ME AND HELP ME GET THROUGH MY DAYS AND I AM SO GREATFUL THAT I DO, BUT WHAT @ THE PEOPLE WHO DON'T HAVE ANYONE TO HELP THEM? THEY ARE OUT THERE.:(
I WANT TO LIVE AGAIN AND ALL I HAVE IS THIS COMPUTER TO SAY WHAT IT IS THAT I NEED TO SAY, BECAUSE IT IS VERY EVIDENT THAT GOING TO DOCTORS ASKING THEM TO HELP FIND WHAT IT IS THAT IS KILLING ME...GETTING VERY OLD AND I AM GETTING NO WHERE, IN THE PROCESS.
AFTER DEALING WITH A CERVICAL SURGERY, I SHOULD AT LEAST HAVE THE RIGHT TO KNOW, IF THERE IS SOMETHING WRONG IN THERE AND NOT BE JUST LEFT IN THE DARK @ IT.
THIS PERSON BELOW, NAMED "JS", IS SUFFERING AND HE, LIKE ME, HAD A CERVICAL DISKECTOMY, BUT IT WAS TOO LATE FOR HIM TO EVER REGAIN HIS LIFE BACK, LIKE IT ONCE WAS..AGAIN.
IT JUST TOOK TOO LONG TO GET ANYONE TO LISTEN TO HIM AND I KNOW HOW HE FEELS. THIS IS ONE OF THE THINGS THAT I AM AFRAID OF, IT TAKING TOO LONG TO FIND THE CULPRIT.
THIS IS JUST AN EXAMPLE OF WHAT CAN HAPPEN AND THIS COULD HAVE BEEN AVOIDED, IF ONLY A DOCTOR WOULD HAVE SEEN THE SIGNS ,B4 IT WAS TOO LATE. HE DIDN'T GET HIS ANSWER FAST ENOUGH AND BY NOT FINDING WHAT IT WAS THAT WAS SO IMPORTANT, HE WOUND UP HAVING PRESSURE ON HIS SPINAL CORD,4 TOO LONG.
IT, ALL CAME DOWN TO THE DOCTOR, NOT TRYING HARD ENOUGH TO GET TO THE BOTTOM OF IT. THIS PROBABLY COULD HAVE BEEN AVOIDED, IF ONLY THE PATIENT, WOULD HAVE BEEN LISTENED TO, IN THE FIRST PLACE .
YEAH, WE DO KNOW OUR BODIES.
JS in SD
Thursday, November 3, 2011

LIFE...CAN BE SO HARD, AT TIMES. JUST LAYING HERE...YEAH, I AM BLESSED TO BE ABLE TO JUST LAY HERE AND OF COURSE, IT SEEMS LUXURIOUS, BUT IT COULDN'T BE FARTHER FROM IT. BEING STUCK ISN'T FUN, BUT IT IS FUNNY HOW SOME PEOPLE LOOK AT BEING DISABLED. THEY THINK IT IS SOMETHING WE SHOULD BE ASHAMED OF AND IT IS, BUT WE CAN'T CHANGE WHAT IS WRONG WITH US...NO, ONLY A DOCTOR CAN CHANGE UR OUTCOME IN THAT FIELD.
I DON'T WANT TO BE DISABLED. NO, I HAVE ALWAYS BEEN ONE TO WORK AND ACTUALLY, I WAS THE ONE WHO LOOOOVED TO WORK. NOW, THAT I AM DISABLED AND AM STUCK TO WHERE I CAN'T DO A GOSH DARN THING...IT IS HARD, IT IS VERY HARD THAT IS...TO NOT TO BE ABLE TO JUST GET UP AND DO WHAT IT IS THAT I WANT. AND PAIN THAT GOES ALONG WITH IT, REALLY MAKES IT SO MUCH HARDER. I KNOW THAT IT IS HARD TO UNDERSTAND FOR SOME, BUT IF UR THERE...U CAN RELATE AND PUT URSELF RIGHT THERE WITH ME.:(
I LAY HERE AND SOMETIMES, I LOOK OUT MY WINDOW AND SEE THE BEAUTIFUL DAY I AM MISSING...AGAIN. ANOTHER DAY OF JUST LAYING HERE MISSING OUT ON THE THINGS THAT I COULD BE DOING. I COULD BE MAKING THIS PLACE LOOK LIKE A LITTLE DOLL HOUSE. INSTEAD, MY HUBBY CLEANS OUR HOUSE AND WORKS 12-14 HOURS A DAY 2. HE HAS WORKED LONGER THAN THAT SOME DAYS, BUT HE NEVER LETS US DO WITHOUT OR LIVE IN A MESS EITHER(THANK U GOD:)) I HAVE TO ADMIT AND GIVE CREDIT TO MY WONDERFUL HUBBY GARY. HE WAS RAISED RIGHT, BY A GOOD MOM AND I LOVE HER FOR HOW SHE TAUGHT HIM TO DO WHAT HE DOES. THANKS NANA 4 TELLING ME WHEN HE SAYS THAT HE WILL DO IT TOMORROW...SAY, "NO, U R GONNA DO IT TODAY"..BUT U KNOW, THERESA, I REALLY HAVEN'T HAD TO USE THAT.:)))
IT MIGHT GET OLD TO HAVE TO LAY HERE, BUT I AM BLESSED..I KNOW THAT. I COULD BE IN THIS SAME PAIN AND NOT HAVE SOME OF THE LUXERIES I HAVE. I AM TRULY THANKFUL FOR EVERYTHING THAT I HAVE..
ALL I WANT IS TO BE PAIN FREE, THEN I WOULD BE UP AND DOING THE THINGS I WANT. IT IS SO FRUSTRATING NOT BEING ABLE TO EVEN TYPE WELL FOR THE CRAMPS IN MY HANDS. MY FEET AND LEGS HURT CONSTANTLY TO WHERE I HAVE TO RUN THE ELECTRIC VIBRATOR IN MY BED. I AM SO BLESSED TO HAVE THAT. I DON'T KNOW WHAT I WOULD DO WITHOUT IT. MY LEGS CRAMP SO MUCH AND MY MUSCLES STAY SO TIGHT. IT FEELS LIKE THE PARTS OF ME THAT BEND ARE CONSTANTLY BEING HIT, SOMEWHAT LIKE HOW IT FEELS TO HAVE YOUR FUNNY BONE HIT OVER AND OVER AGAIN. I DESCRIBE IT LIKE THAT BECAUSE EVERYONE KNOWS HOW IT FEELS TO HAVE YOUR FUNNY BONE HIT. I MUST SAY THAT IT IS ONE OF THE MOST AGGRAVATING SYMPTOMS THAT I HAVE.
NOW, I HAVE SO MANY THAT IT WOULD BE UTTERLY IMPOSSIBLE TO LIST THEM ALL. I CAN EXPLAIN THEM AS I HAVE THEM, BECAUSE MY MEMORY IS SEEMING TO BE GIVING ME MORE PROBLEMS. MY BRAIN FEELS NUMB AND IT IS SORT OF LIKE I AM A ZOMBIE. I HATE IT. I MUST BE OF A RARE BREED, BUT I HONESTLY HATE IT. I AM ONE OF THOSE PEOPLE WHO LIKE TO THINK FOR THEMSELVES AND DO FOR THEMSELVES.
OHH, I AM EXPERIENCING A DEEP PAIN IN MY RIGHT SHOULD AND IT GOES ALL THE WAY UP MY NECK. I GUESS, I COULD SAY..RIGHT NOW, MY NEXT AGGRAVATING SYMPTOM WOULD BE THAT YOU NEVER KNOW WHAT IS COMING NEXT.
WHILE THE SHOULDER PAIN IS STILL LOCKING MY NECK AND CRAMPING. I AM HAVING PRESSING HEAD PAIN LIKE SOMEONE IS PUSHING MY HEAD DOWN. IT IS A HORRIBLE FEELING, WHEN IT FEELS LIKE SOMEONE HAS THEIR THUMB AND IS PRESSING IT HARD INTO UR HEAD...YOWCH!..I HATE THAT.:(((( MY EARS ARE RINGING AND MY EYES ARE GETTING SOMEWHAT BLURRY. I WOULD SAY THAT I AM HAVING SOME SERIOUS SYMPTOMS...WOULDN'T YOU? THIS IS EVERY SINGLE DAY AND IT GETS OLD WHEN U DON'T KNOW WHAT IS COMING...BUT, I AM STILL IN THIS SAME BOAT. LAYING HERE AFTER 6 YRS OF MY LIFE HAS JUST FADED INTO THIS HOLE THAT I LIVE IN. WELL, THAT IS WHAT I CALL IT. IT IS A HOLE. TO ME, BECAUSE I HAVE PILLOWS THAT ARE ON EACH SIDE THAT I LEAN MY ARM ON.
MY HANDS ARE HAVING PINS/NEEDLES AND I NOTICED THAT I HAVE CLOSED ONE EYE TO SEE WHAT I AM TYPING. I AM NOT GOING TO LIE. I AM SCARED AND I AM PRAYING TO THE LORD THAT HE WILL HEAL ME SOON AND MAKE ME BETTER.
LIFE SEEMS DREARY AND IT IS OH SO WEIRY FOR ME, TO LAY HERE ALL THE TIME. I USED TO BE SO ACTIVE AND DID SO MANY THINGS. I SANG EVERYWHERE AND LOVED IT. I SANG FOR PAGAENTS, TALENT SHOWS AND JUDGED ALL SORTS OF ENTERTAINMENT. I LOVED BEING OUT AND SINGING. I FEEL THAT, THAT PART OF ME HAS BEEN LOST ,SOMEHOW. I DON'T KNOW THAT PART OF ME ANYMORE AND THAT IS HARD FOR ME TO FACE. I USED TO PLAY MY GUITAR (OVATION) AND SET ON THE BACK PORCH, BUT THAT IS A DREAM NOW, FOR MY HANDS TO WELL TO GET THIS OUT.
I AM GOING TO GO FOR NOW. I DON'T HAVE THE LUXURY OF JUST JUMPING UP AND DOING WHAT I WANT, ANYMORE. I HAVE TO LAY HERE AND LAY HERE. YES, IT DOES GET VERY OLD AND TO ME, THIS IS NOT LIVING, BUT I WILL FIGHT ANOTHER DAY...AND WHO KNOWS, MAYBE I WILL GET TO GET OUT OF THIS BED ONE DAY. "LORD WILLING" THAT IS.
KEEP ME IN UR PRAYERS PLEASE THAT I WILL GET WELL I DO WANT TO THANK EVERYONE WHO HAS PRAYED FOR ME.:)) I JUST WANT MY LIFE TO BE A BLESSING TO OTHERS...THAT IS :))) ALL I WANT..IS TO HELP OTHERS. SO MAYBE GOD WILL LET ME GET WELL AND LET MY LIGHT SHINE FOR HIM. GOD BLESS ALWAYS.;)))<3 Karen
Saturday, October 15, 2011
MYOFASCIAL PAIN SYNDROME(OMOHYOIDEUS-4 patients reports)
 The JOURNAL OF CRANIOMANDIBULAR PRACTICE June '84-Aug. 'b4, Vol. 2, No. 3
The Omohyoideus Myofascial Pain
Syndrome: Report of Four Patients
|





Subscribe to:
Posts (Atom)
The success of back surgeries is determined by a couple of factors. The most obvious is the skill of the surgeon. A good surgeon knows when it makes sense to operate and when it does not. They also know how to minimize or eliminate secondary problems resulting from the surgery itself. Another factor is how well the person that had the surgery follows the doctors instructions following the surgery. This includes not trying to push things too quickly as well as doing the physical therapy that is needed to recover. A final factor is, unfortunately, just luck. Some people will come back well and others will not. Know one really knows why some people respond better than others.
I DO AGREE THAT BY THE TIME THE DOCTORS DO GET A CLUE, THEN IT COULD BE TOO LATE. I CAN'T STAND TO HARDLY BRUSH MY OWN TEETH...I CRY. THERE IS SOMETHING VERY VERY WRONG HERE, BUT I CAN'T SEEM TO GET ANYWHERE. I HAVE BEEN TO DOCTORS, BUT MUST SAY THAT THEY DON'T TAKE YOU THAT SERIOUSLY. NO, THEY THINK YOU ARE FULL OF HOT AIR AND JUST WANT ATTENTION. "NOT"..NO, UNFORTUNATELY, WHAT I HAVE IS REAL. IT IS VERY PAINFUL AND I TRY...I REALLY DO TRY TO GET THROUGH EACH DAY WITH A SMILE AND MOST OF THE TIME...I HAVE TO GRIN AND BEAR IT AND HAVE TO ADMIT THAT I AM SCARED.
I DO KNOW THAT I LIVE IN A SMALL TOWN AND THAT MAKES IT HARD AND I HAVE TO TRAVEL. I DON'T LIVE WHERE IS SOMEONE WHO COULD FIX ME. I HAVE TO GO TO THEM AND DO YOU KNOW WHAT THAT FEELS LIKE, FOR SOMEONE THAT EVERY LITTLE BUMP IN THE ROAD, IS LIKE SOMEONE ACTUALLY HURTING YOU?
ALL I WANT IS TO BE TAKEN SERIOUSLY AND FIND THAT DOCTOR WHO IS GOING TO PUT ME BACK TOGETHER AGAIN. AFTER THAT SURGERY OF THE ACD & F SPINAL DISKECTOMY OF MY C5-C6, MY LIFE HAS DONE NOTHING, BUT GO STEADILY DOWNHILL. SOMETHING IS WRONG IN THERE AND IF THEY CAN'T SEE BEHIND MY TITANIUM PLATES AND I HAVE BEEN CHECKED EVERYWHERE ELSE IN MY BODY, I THINK. THEN, I THINK IT SHOULD BE LOOKED INTO AND DONE. DON'T YOU?
I HAVE GOT TO WHERE I CAN'T DO ANYTHING AND LIVE IN THE BED..80-90% OF THE TIME. I HAVE BEEN DIAGNOSED WITH DEGENERATIVE DISC DISEASE, SPONDYLOSIS AND SPINAL STENOSIS....WHY? WHERE DID IT COME FROM, WHEN THEY TOLD ME THAT ALL I HAD AT THE TIME OF SURGERY WAS A RUPTURED PETRUSION? THEY HAVE EVEN DOCUMENTED THAT I HAVE A T3-T4 COMPRESSED FRACTURE...."WHAT?" WHAT IS GOING ON IN MY BODY? I WANT TO FIND OUT NOW. I AM TIRED OF LIVING LIKE THIS!!!
GOD BLESS ALWAYS.:)))<3 Karen